
Precautions for Manual Therapy of the Lumbar Spine and Pelvis
This blog post article is an overview of the precautions and contraindications for manual therapy to the lumbar spine and pelvis. For more complete coverage of the structure and function of the low back and pelvis, Kinesiology – The Skeletal System and Muscle Function, 3rd ed. (2017, Elsevier) should be consulted.
The low back and pelvic region contains a number of neurovascular structures (nerves, arteries, and veins) whose locations are important to know because they contraindicate deep pressure. These structures are located both anteriorly and posteriorly (Fig. 48). However, even though caution is called for in the vicinity of these structures, it should not prevent therapeutic work entirely. A good guideline when working near any neurovascular structure is to begin with light to medium pressure before transitioning to deeper pressure. Knowledge of the anatomy of the region can allow work to be performed therapeutically and safely.
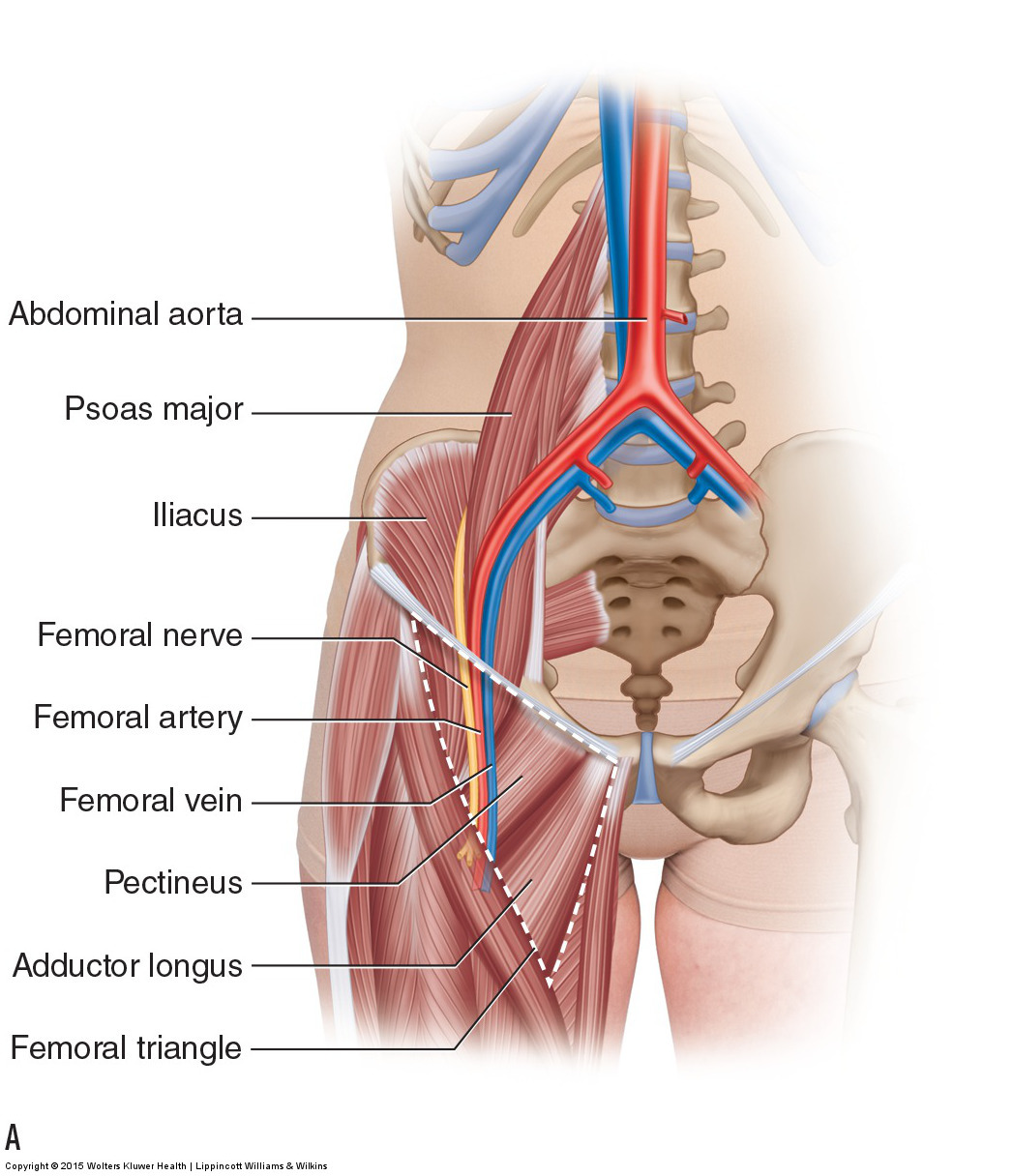
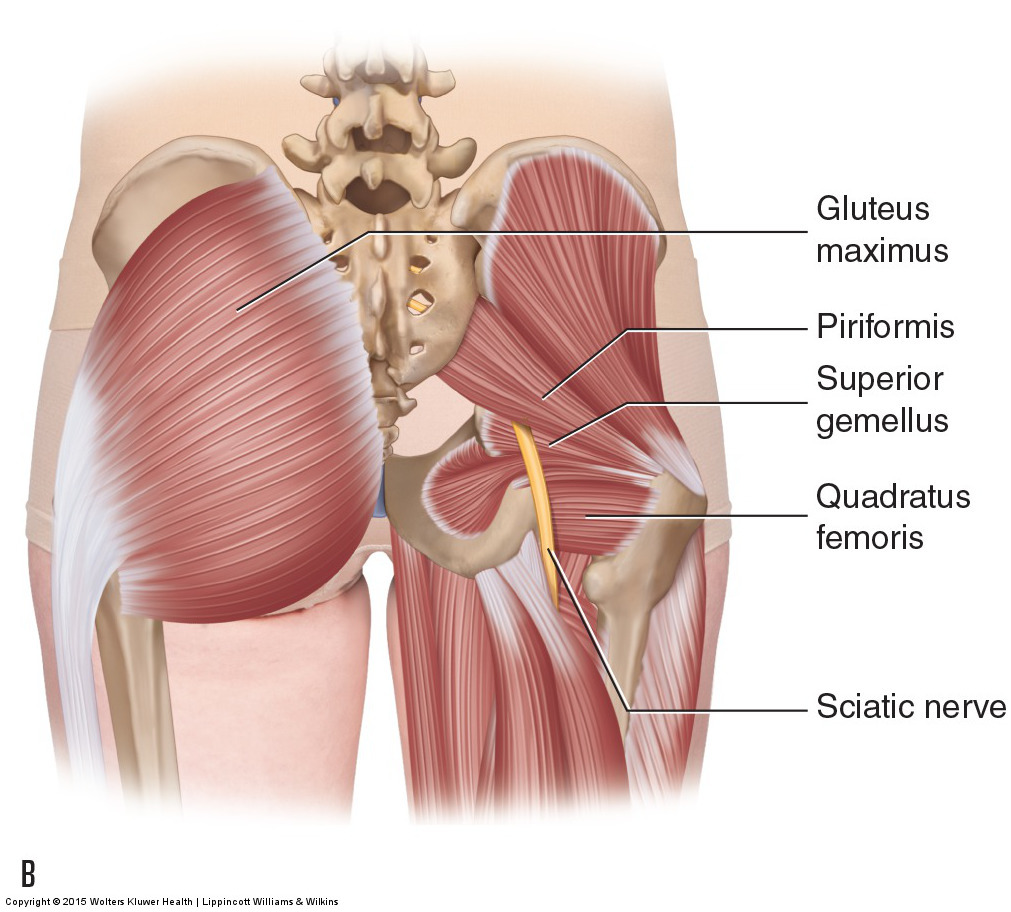
Figure 48. Neurovascular structures of the low back and pelvis. (A) Anterior view showing the abdominal aorta and the femoral triangle containing the femoral nerve, artery, and vein. (B) Posterior view showing the sciatic nerve.
Note: Gluteal Work and Referral Symptoms
Pain or other referral symptoms experienced into the lower extremity when applying pressure to the gluteal region can result from pressure directly on the sciatic nerve. However, pressure to the gluteal region in the vicinity of the sciatic nerve can also refer symptoms into the lower extremity because of trigger point (TrP) referral. Therefore, it can be difficult to be certain of the cause of the referral. Referral caused by direct nerve pressure tends to feel like a shooting pain; however, this is not always the case. Consulting a TrP referral illustration may help. If your client’s pain falls within the typical TrP referral pattern, it is more likely that the pain is a TrP referral, but this is not definite. If the referral does not coincide with the typical TrP referral pattern, then you are most likely pressing directly on the sciatic nerve and should move your pressure slightly so as to remove pressure from the nerve. When in doubt, it is always wise to be cautious and change the location of your pressure.
Note: Working with the Client Prone
Many clients have a difficult time spending long periods of time lying prone because this position causes the lumbar spine to be unsupported, placing stress upon the posterior musculature and ligaments. This can be true for anyone, but is especially true if the client is experiencing an acute condition of the low back. This is ironic and unfortunate because the soft tissue work necessary to help alleviate a low back problem is best done with the client prone. When confronted with this circumstance, the therapist has three choices:
- Limit the time that the client spends prone.
- Place a small roll under the client’s lumbosacral area.
- Work with the client side-lying instead (and place a small pillow between the client’s thighs/knees.
Also of value is to have the client stretch her low back as soon as she gets up from the prone position. The yoga Child’s (or Restorative) Pose is an excellent way to accomplish this (see accompanying figure).

Lateral View of the Child’s (Restorative) Pose
Anterior Structures of the Lumbar Spine/Pelvis: Abdominal Aorta
The abdominal aorta is located within the abdominal cavity, running along the midline of the anterior surfaces of the vertebral bodies and discs (see Fig. 48A). Because it is located so deeply, it is rarely accessed. However, pressure can be placed upon it if the therapist is working the belly of the psoas major within the abdomen and is working slightly too medially. For this reason, when palpating for and working the psoas major, it is important to be mindful of the location of the aorta and to make sure that no pressure is being placed upon it. It is usually easy to know when the fingers are pressing on the aorta, or any artery for that matter, because a pulse can be felt. If a pulse is felt, move laterally off the aorta.
Anterior Structures of the Lumbar Spine/Pelvis: Femoral Triangle
The femoral triangle is the name given to the region in the proximal anterior thigh; immediately distal to the inguinal ligament; and overlying the adductor longus, pectineus, and iliopsoas muscles. Within the femoral triangle are the femoral nerve, femoral artery, and femoral vein (see Fig. 48A). It is important to be mindful of these structures when work is being done to the proximal attachments of the hip flexor and adductor musculature. If a pulse is felt, you are on the femoral artery. It is not necessary to stop working. Instead, either slightly move your palpating fingers or try to gently displace the vessel to one side or the other and continue working in that spot. When first applying pressure in this region, be sure to begin with lighter pressure because deep pressure could compress the artery and block its blood circulation, thereby blocking palpation of its pulse as well.
If pressure is applied in this region and the client feels a sharp pain that shoots into the anterior thigh, then it is likely that the femoral nerve is being compressed. As with the femoral artery, either slightly move your palpating fingers or try to gently displace the nerve by accessing from one side or the other and continue working in that spot.
Posterior Structures of the Lumbar Spine/Pelvis: Sciatic Nerve
The sciatic nerve is the largest nerve in the human body; it is approximately a quarter inch in diameter. It emerges in the gluteal region between the piriformis and superior gemellus muscles (although variations are common in which part or all of the nerve emerges through or superior to the piriformis) (see Fig. 48B). It then runs superficial to the rest of the deep lateral rotator muscles (and deep to the gluteus maximus) in the gluteal region before entering the thigh. Because the sciatic nerve is deep to the gluteus maximus muscle, it is not very superficial and therefore not easily injured with soft tissue work. However, deeper work can translate to the sciatic nerve and the therapist should be mindful of this, especially when performing deep work on the quadratus femoris muscle.
Precautions Regarding Motions of the Lumbar Spine and Pelvis
Another caution should be mentioned, even though it does not involve an anatomic structure per se. When treating the client’s low back, be aware that many clients do not tolerate well any extension beyond anatomic position and/or any extreme or fast rotation motions. This is especially true with elderly clients, but it may also be true for middle-aged or younger clients. The lumbar spine has limited rotation ranges of motion. Further, rotation and extension motions cause the surfaces of the facet joints to approximate each other; if they are injured or irritated in any way, and/or if there are degenerative joint changes (osteoarthritis), this can result in pain. For this reason, it is always wise to be aware of this possibility. When stretching or otherwise moving the client, it is advisable to increase these ranges of motions gradually over the span of several visits if necessary.
At the hip joint, caution must be exercised whenever the client’s thigh is moved into flexion combined with adduction and medial rotation. This is especially important for clients who have had hip replacement surgery.
Note: This is the eighth in a series of 8 blog post articles on the anatomy and physiology of the lumbar spine and pelvis.
The blog post articles in this series are:
- Bones of the Lumbar Spine and Pelvis
- Joints of the Lumbar Spine (disc & facet) and Pelvis
- Motions of the Joints of the Lumbar Spine
- Motions of the Joints of the Pelvis
- Muscles of the Lumbar Spine
- Muscles of the Pelvis
- Ligaments of the Lumbar Spine and Pelvis
- Precautions for Manual Therapy of the Lumbar Spine and Pelvis
