Signs and symptoms of spinal joint dysfunction
A hypomobile spinal joint usually causes no pain or loss of gross range of motion of the spinal region in which it is located. Because of compensatory hypermobile joints, even two or perhaps three hypomobile joint levels may be asymptomatic. However, once the number of hypomobile joints is too many for the adjacent spinal joints to compensate, gross range of motion will decrease and the client/patient gross range of motion will decrease. Depending upon the client’s/patient’s activity level, the client/patient might or might not feel tight and notice the decreased spinal motion. Unfortunately, by this time, the hypomobile segments have probably been present for months if not years. The only reliable sign of an individual hypomobile spinal joint is decreased motion upon motion palpation of that segmental level. It is possible that deep palpation of the soft tissues of the hypomobile spinal joint might reveal tight musculature and/or fascial adhesions.
Similarly, an individual hypermobile spinal joint will also usually not be symptomatic. If a number of joint levels are hypermobile, then increased range of motion will be present.
Assessment/Diagnosis of spinal joint dysfunction

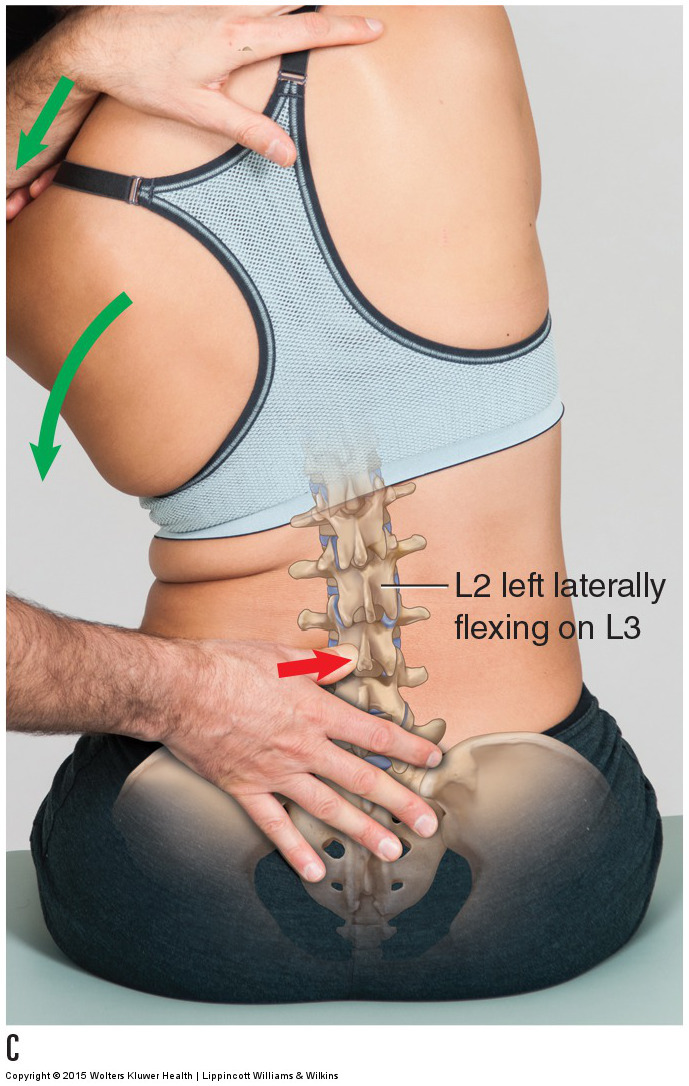
Motion palpation assessment (and joint mobilization treatment) of the lumbar spine with the client seated. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Assessment/diagnosis of spinal joint dysfunction, whether it is a hypomobility or a hypermobility, is done via motion palpation. Motion palpation is accomplished by the therapist using one hand to pin/stabilize one vertebra (occasionally the client’s/patient’s body weight can function to stabilize the vertebra) while the other hand contacts and moves an adjacent vertebra. Pinning one vertebra and moving the adjacent one causes motion at the joint located between the two vertebrae. At the end of passive range of motion, the therapist adds a gentle slow force for less than a second. This challenges the joint to move into joint play. The therapist should be able to palpate/feel a full range of motion of the joint as well as a healthy spring/bounce at the end-feel of the joint motion. If the motion is decreased and/or if the end-feel is hard, the joint is hypomobile. If the motion is excessive and/or the end-feel is mushy, the joint is hypermobile. Each of the joints of the spine can be motion palpated in this manner. It is typical to perform the motion palpation stroke 1-2 times at each segmental joint level of the region of the spine being assessed. The order in which the joints are assessed does not matter. The therapist can start at the lower aspect of the region and work their way upward, or start at the upper end and work their way downward. What is important is that each and every joint is assessed.
Each region of the spine can be assessed into any range of its motion. In the cervical region, with the client/patient supine, the therapist uses the radial side of the index finger to pin/stabilize the lower vertebra of the joint while the other hand moves into right lateral flexion the head and vertebrae superior to the pinned vertebra relative to the pinned vertebra.
In the thoracic spine, with the client/patient prone, the therapist places a gentle force on the spinous process from posterior to anterior, assessing the joint’s ability to move into extension. Or presses against the spinous process laterally assessing rotation motion. Or presses posteriorly to anteriorly onto the transverse process, assessing rotation motion of the spine at that segmental level.
The joints of the rib cage can be assessed with the client/patient seated; the therapist flexes and rotates the client’s/patient’s trunk toward the therapist, and then runs a thumb downward along the angles of the ribs, feeling for a rib that has not moved into a smooth line along with the other ribs.
The lumbar spine can also be assessed with the client/patient seated by laterally flexing the client’s/patient’s trunk while pinning against a lumbar spinous process; this focuses and challenges the lateral flexion motion at the joint directly above the pinned vertebra. Even though joint dysfunction is usually asymptomatic and does not cause the client/patient pain, when a hypomobile spinal joint is challenged to move with motion palpation assessment technique, the client/patient often does experience discomfort. This is further confirmation that the joint is hypomobile.
It is also common for the therapist to statically palpate the position of the vertebrae. Usually, the spinous processes are palpated. If one vertebra is misaligned relative to the adjacent vertebrae, then clearly that bone is being held out of its anatomic position. For example, if T7’s spinous process is rotated to the right relative to the spinous processes of T6 above and T8 below, then the assumption is that there is an asymmetry of tension forces by soft tissues that are holding that vertebra in its misaligned position. If this is the case, then it is likely that the soft tissues with increased tension that are pulling the vertebra in one direction, for example the spinous process of T7 to the right, will restrict the motion of the vertebra in the opposite direction: in this example restrict the motion of the spinous process into left rotation. Note: Rotation of a vertebra is named for the orientation of the anterior surface of the body, therefore restricted motion of a spinous process to the left is named as restricted right rotation.
Differential Assessment of spinal joint dysfunction
Assessment of spinal joint dysfunction is straightforward; if motion palpation reveals that the joint’s motion is restricted or excessive, the assessment of joint dysfunction can be made. The more important question is: What is causing the joint dysfunction? Bones are passive elements; if their motion is altered, there must be a reason. Therefore, whenever spinal joint dysfunction is found, look for other conditions that can be causing the dysfunction and/or look for habitual postures and movement patterns that the client/patient is assuming that might be contributing to the problem.
