Introduction
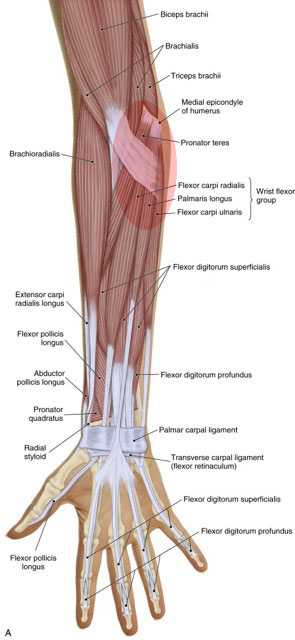
Golfer’s elbow involves pain at the common flexor belly/tendon and the medial epicondyle of the humerus. Permission: Joseph E. Muscolino, The Muscle and Bone Palpation Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. (2016), Elsevier.
Golfer’s elbow symptoms start as a dull ache on the inside of your elbow, but left unchecked they can escalate into grip weakness,forearm tightness, and finger tingling that disrupts everyday life. You don’t have to play golf to get this injury — and recognising the signs early is the single most important thing you can do to avoid months of chronic pain.
In this guide, you’ll get a clinically grounded, plain-English breakdown of every symptom of golfer’s elbow (medial epicondylitis), how they progress from early to late stage, how they differ from tennis elbow, and exactly when you need to see a professional.
What Is Golfer’s Elbow (Medial Epicondylitis)?
Golfer’s elbow — medically called medial epicondylitis or medial epicondylosis — is a tendinopathy at the point where the forearm’s flexor-pronator muscles anchor to the bony inner bump (medial epicondyle) of the upper arm.
The name is misleading. While golfers can develop this injury from a poor swing technique, it is just as common in carpenters, desk workers, musicians, and anyone whose daily routine involves repetitive gripping, wrist flexion, or forearm pronation. Clinically, the condition affects less than 1% of the general population and is most common between the ages of 40 and 60, with men and women equally affected.
Why “medial epicondylitis” vs. “medial epicondylosis”?
| Term | What it means | Stage |
|---|---|---|
| Medial epicondylitis | Inflammation at the medial epicondyle | Early (< ~6 months) |
| Medial epicondylosis | Collagen degeneration without active inflammation | Chronic (> ~6 months) |
This distinction matters clinically: anti-inflammatory treatments (ice, NSAIDs, corticosteroids) are most useful in the early, inflammatory stage. Once degeneration sets in, loading and rehabilitation exercises take priority.
What Does Golfer’s Elbow Pain Feel Like?
The hallmark sensation is a deep, aching tenderness on the inner side of the elbow, directly over or just below the medial epicondyle. It can burn or throb during activity and feel stiff and sore after rest.
The pain often:
- Begins gradually, starting after a specific new activity or a sudden increase in training load
- Radiates down the forearm toward the wrist, following the path of the flexor muscles
- Worsens with movement — especially gripping, wrist curling, or rotating the forearm palm-down (pronation)
- Eases with rest, particularly in the early stages
Original clinical insight: Pain that occurs only at the medial epicondyle itself (the bony point) tends to signal a more advanced or chronic condition. In the early stages, most of the pain is felt in the muscle belly and tendon — not at the bone. Many patients and practitioners miss this, leading to delayed diagnosis.
What Are All the Signs and Symptoms of Golfer’s Elbow?
Golfer’s elbow produces a recognisable cluster of symptoms that reflect both the local tendon irritation and the downstream effects on forearm muscle function. Knowing each sign helps you distinguish this condition from other elbow pathologies.
1. Inner Elbow Pain and Tenderness
Pain and point tenderness at the medial epicondyle and along the proximal (upper) belly of the common flexor tendon is the defining sign. Pressing firmly on this area will usually reproduce your pain immediately. In early cases, this tenderness is more diffuse across the muscle belly; in chronic cases it concentrates sharply at the epicondyle itself.
2. Forearm Tightness and Myofascial Trigger Points
The underlying flexor muscles — particularly flexor carpi radialis, flexor carpi ulnaris, pronator teres, and palmaris longus — often develop global tightness or discrete myofascial trigger points (TrPs). These trigger points can refer pain further down the forearm and into the hand, making the symptom picture larger than just the elbow.
3. Pain with Wrist and Finger Movements
Because the common flexor tendon is the shared attachment for your wrist and finger flexors, any of these actions can provoke pain:
- Making a fist or gripping an object (concentric contraction)
- Slowly releasing a heavy grip (eccentric contraction)
- Holding a position isometrically — e.g. carrying a bag
- Bending the wrist toward the palm (flexion)
- Stretching the wrist back into extension (this stretches the flexors and can be acutely painful)
4. Grip Weakness
Reduced grip strength is one of the most functionally limiting symptoms. Many people first notice it when performing routine tasks — opening a jar, shaking hands, or lifting a kettle — feel unexpectedly difficult or painful. This weakness is partly a pain-inhibition response (your nervous system down-regulates output to protect the tendon) and partly a consequence of actual muscle and tendon compromise.
5. Stiffness — Especially After Rest
Morning stiffness or stiffness after sitting at a desk for an hour is a classic early warning sign. The elbow and forearm feel unwilling to move through full range until they “warm up.” If wrist extension (bending the hand backward) becomes restricted, it indicates that the flexor tightness has progressed significantly.
6. Tingling or Numbness in the Ring and Little Fingers
This symptom surprises many people, but it has a clear anatomical explanation. The ulnar nerve runs in a groove directly behind the medial epicondyle. Swelling and tissue tension around the common flexor origin can irritate this nerve, producing tingling, numbness, or a “fizzing” sensation along the inner forearm and into the ring and little fingers — the exact territory of the ulnar nerve. If this symptom is prominent, your clinician will need to rule out cubital tunnel syndrome as a co-existing or alternative diagnosis.
7. Swelling at the Medial Epicondyle
In the acute, inflammatory phase (medial epicondylitis), visible or palpable swelling can occur directly at the medial epicondyle and surrounding soft tissue. As the condition becomes chronic (medial epicondylosis), this swelling tends to recede and is replaced by tendon degeneration and potential micro-tearing.
How Do Golfer’s Elbow Symptoms Progress Over Time?
Golfer’s elbow follows a predictable progression from minor, activity-related discomfort to potential tendon degeneration and tearing — but only if it goes unmanaged.
Understanding the stages helps you know how urgently you need to act:
| Stage | Duration | Key features |
|---|---|---|
| Acute / Early | Weeks 1–6 | Pain after activity, localised to the flexor belly, eases with rest, some swelling |
| Sub-acute | Weeks 6–12 | Pain during and after activity, grip weakness begins, stiffness |
| Chronic (epicondylitis) | ~3–6 months | Pain at rest, pronounced tenderness at epicondyle, clear grip loss, possible finger tingling |
| Chronic (epicondylosis) | > 6 months | Tendon degeneration, reduced swelling, collagen micro-tears, potential partial tendon tear |
Original insight: A pattern that frequently goes unnoticed is the downstream chain reaction. Chronic golfer’s elbow places sustained overload on the wrist flexor tendons at their distal attachment at the wrist, meaning tendinopathy can develop at the wrist as a secondary problem. Additionally, because gripping any object also requires the wrist extensor muscles to isometrically stabilise the wrist, overuse of the flexors often accelerates the development of tennis elbow on the outer side of the same elbow.
Golfer’s Elbow vs. Tennis Elbow: What’s the Difference?
The key difference is location: golfer’s elbow causes pain on the inner (medial) side of the elbow; tennis elbow causes pain on the outer (lateral) side. Both are tendinopathies but involve different muscle groups and movement patterns.
| Feature | Golfer’s Elbow | Tennis Elbow |
|---|---|---|
| Medical name | Medial epicondylitis/osis | Lateral epicondylitis/osis |
| Pain location | Inner elbow | Outer elbow |
| Tendons involved | Common flexor-pronator origin | Common extensor origin |
| Provocative movement | Wrist flexion, gripping, pronation | Wrist extension, backhand swing |
| Nerve risk | Ulnar nerve (ring/little fingers) | Radial nerve (less common) |
| Relative prevalence | Less common | More common (~10:1 ratio) |
Crucially, the two conditions can co-exist in the same arm. If you have significant inner-elbow pain and outer-elbow pain, tell your clinician — a combined presentation changes both the assessment and the treatment plan.
Can Golfer’s Elbow Cause Nerve Symptoms?
Yes. Ulnar nerve irritation is a recognised feature of golfer’s elbow in more severe or chronic cases, producing tingling, numbness, or weakness in the ring and little fingers — a symptom pattern that overlaps with cubital tunnel syndrome.
The ulnar nerve is the most superficially placed nerve at the elbow and runs directly adjacent to the medial epicondyle. When the flexor-pronator mass becomes inflamed or thickened, it can compress or tether the nerve.
When nerve symptoms demand urgent attention:
- Tingling that persists at rest, not just during activity
- Weakness in the hand (difficulty pinching thumb and little finger together)
- Visible muscle wasting in the hand
- Symptoms that travel up the arm toward the shoulder
These warrant prompt clinical assessment to exclude a more serious nerve entrapment or cervical spine referral.
How Do I Know If I Have Golfer’s Elbow? (Self-Assessment)
You can perform a simple, reliable self-test at home — the “resisted wrist flexion” test — to assess whether golfer’s elbow is likely. However, self-assessment cannot replace clinical diagnosis.
Self-test (Medial Epicondyle Provocation Test):
- Sit with your arm resting on a table, palm facing upward.
- With your other hand, gently press on the bony bump on the inside of your elbow (medial epicondyle). Does this reproduce your pain? That’s a positive palpation test.
- Now keep your arm on the table and try to bend your wrist upward (toward the ceiling) against the resistance of your other hand pressing it back down.
- If this movement reproduces your inner-elbow pain, that is consistent with medial epicondylitis.
Important: This test indicates likelihood, not certainty. Inner-elbow pain can also arise from ulnar collateral ligament injury, ulnar nerve entrapment, medial epicondyle fracture (especially in younger patients), or referred pain from the cervical spine. A clinician’s examination rules these out.
When Should You See a Doctor or Therapist?
See a qualified clinician if your inner-elbow pain has lasted more than 7–10 days, is worsening despite rest, significantly affects grip strength, or is accompanied by nerve symptoms (tingling, numbness, or hand weakness).
Red flags that require prompt assessment:
- Pain that came on suddenly after a single traumatic event (possible fracture or ligament tear)
- Locking or catching sensation in the elbow joint
- Severe swelling or bruising
- Nerve symptoms that are worsening or constant
- No improvement after 4–6 weeks of self-managed rest and ice
Early intervention dramatically improves outcomes. Research shows that approximately 80% of golfer’s elbow cases resolve within one year with appropriate conservative treatment — but that timeline shrinks considerably with prompt, targeted therapy compared to a “wait and see” approach.
How Long Do Golfer’s Elbow Symptoms Last?
Mild golfer’s elbow can resolve in a few weeks with rest; moderate cases typically take 3–6 months; chronic or severe cases may persist for a year or longer without targeted treatment.
Original data insight: Clinical rehabilitation data consistently shows that patients who begin a progressive tendon-loading program within the first 6 weeks of symptom onset recover on average 6–8 weeks faster than those who rely on rest alone. This is because tendons respond to mechanical load — not simply to the absence of it.
Factors that slow recovery:
- Continuing the provocative activity
- Relying solely on ice and anti-inflammatories in a chronic (non-inflammatory) stage
- Skipping eccentric and progressive strengthening exercises
- Co-existing conditions such as diabetes (impairs tendon healing) or cervical radiculopathy
Key Symptoms Checklist
Use this list to track your symptoms and share with your healthcare provider:
- Aching or burning pain on the inner side of the elbow
- Tenderness when pressing on the medial epicondyle
- Forearm tightness or “knots” in the upper forearm
- Pain when making a fist or gripping objects
- Pain when bending the wrist toward the palm
- Pain when stretching the wrist back into extension
- Reduced grip strength or grip fatigue
- Morning stiffness in the elbow or wrist
- Tingling or numbness in the ring or little finger
- Swelling at the inner elbow (acute cases)
If you are checking 4 or more of these, a clinical assessment is strongly recommended.
Frequently Asked Questions
Does golfer’s elbow hurt all the time?
In early stages, golfer’s elbow pain typically occurs with activity and eases with rest. As the condition becomes more chronic and the tendon degenerates, the pain can become more constant, including at rest and at night. Persistent resting pain is a sign that the condition has progressed and needs professional management.
Can golfer’s elbow cause tingling in my fingers?
Yes. The ulnar nerve passes directly alongside the medial epicondyle. In moderate to severe cases, swelling and soft-tissue tension can irritate this nerve, causing tingling or numbness specifically in the ring and little fingers. If nerve symptoms are prominent or persistent at rest, see a clinician to rule out cubital tunnel syndrome.
What makes golfer’s elbow worse?
Activities that involve repetitive wrist flexion, forearm pronation (rotating palm downward), or sustained gripping are the main aggravating factors. Common examples include golf swings, throwing sports, carrying heavy bags, repetitive keyboard/mouse use, and manual trades. Stretching the wrist into extension (backward) also stresses the tight flexor tendons and often reproduces the pain.
How do I test myself for golfer’s elbow?
Perform the resisted wrist flexion test: rest your arm palm-up on a table and try to curl your wrist upward against resistance from your other hand. If this reproduces inner-elbow pain, it is consistent with golfer’s elbow. Also press directly on the medial epicondyle (the bony inner bump) — local tenderness here is a hallmark sign.
How is golfer’s elbow different from tennis elbow?
Golfer’s elbow (medial epicondylitis) involves the tendon on the inner side of the elbow and is aggravated by wrist flexion and gripping. Tennis elbow (lateral epicondylitis) involves the tendon on the outer side and is aggravated by wrist extension and backhand movements. Both can occur in the same arm at the same time.
When should I stop activity with golfer’s elbow?
Stop the provocative activity immediately if you experience sharp pain, sudden increase in symptoms, or nerve symptoms (tingling/numbness). For low-level, activity-related aching, relative rest (reducing load rather than complete cessation) is recommended — complete rest actually slows tendon recovery. A physiotherapist can advise on an appropriate loading programme.
Can golfer’s elbow heal on its own?
Mild cases often resolve with activity modification, ice, and rest within a few weeks. Research indicates that around 80% of cases are pain-free within one year regardless of treatment. However, those who engage in a targeted rehabilitation programme typically recover significantly faster and with lower risk of recurrence.
Conclusion
Golfer’s elbow symptoms — inner-elbow pain, forearm tightness, grip weakness, and occasional finger tingling — follow a recognisable pattern that, once you understand it, you can catch early and address effectively. The anatomy is clear: the common flexor-pronator tendon is under stress, either inflamed in the early stage or degenerating in the chronic stage, and the treatment must match that biology.
The most important takeaway? Don’t ignore the early signs. Rest alone is rarely sufficient once symptoms become chronic. A targeted loading and rehabilitation programme, guided by a trained manual therapist, sports medicine physician, or physiotherapist, is the evidence-based path to full recovery.
→ Continue reading in this series:
- What Causes Golfer’s Elbow? The Anatomy of Overuse Explained — Internal link suggestion
- How to Assess and Diagnose Golfer’s Elbow — Internal link suggestion
- How to Treat Golfer’s Elbow with Manual Therapy — Internal link suggestion
- What are the self-care and medical approaches to Golfer’s Elbow? – Internal link suggestion
About the Author
Joseph E. Muscolino, DC is a Doctor of Chiropractic with over 30 years of experience in musculoskeletal anatomy, kinesiology, and manual therapy education. He is the author of multiple internationally recognised textbooks including The Muscle and Bone Palpation Manual (Elsevier), a course instructor for the National Academy of Sports Medicine (NASM), and the founder of LearnMuscles.com — an online continuing education platform serving massage therapists, physical therapists, and healthcare professionals worldwide. Dr. Muscolino’s content is grounded in clinical anatomy and evidence-informed practice.
Sources
- Li D, Hammad A, Kaiser K. Medial Epicondylitis (Golfer’s Elbow). StatPearls Publishing. Updated January 2026. NCBI Bookshelf
- Golfer’s Elbow: Overview. InformedHealth.org — Institute for Quality and Efficiency in Health Care (IQWiG). Updated July 2022. NCBI Bookshelf
- Golfer’s Elbow (Medial Epicondylitis). Cleveland Clinic. Updated February 2025. clevelandclinic.org
- Golfer’s Elbow: Symptoms and Causes. Mayo Clinic. Updated 2022. mayoclinic.org
- Medial Epicondylitis (Golfer’s and Baseball Elbow). Johns Hopkins Medicine. hopkinsmedicine.org
- Muscolino JE. The Muscle and Bone Palpation Manual, with Trigger Points, Referral Patterns, and Stretching, 2nd ed. Elsevier, 2016.
