Attachments and Actions of the Coccygeus and Levator Ani
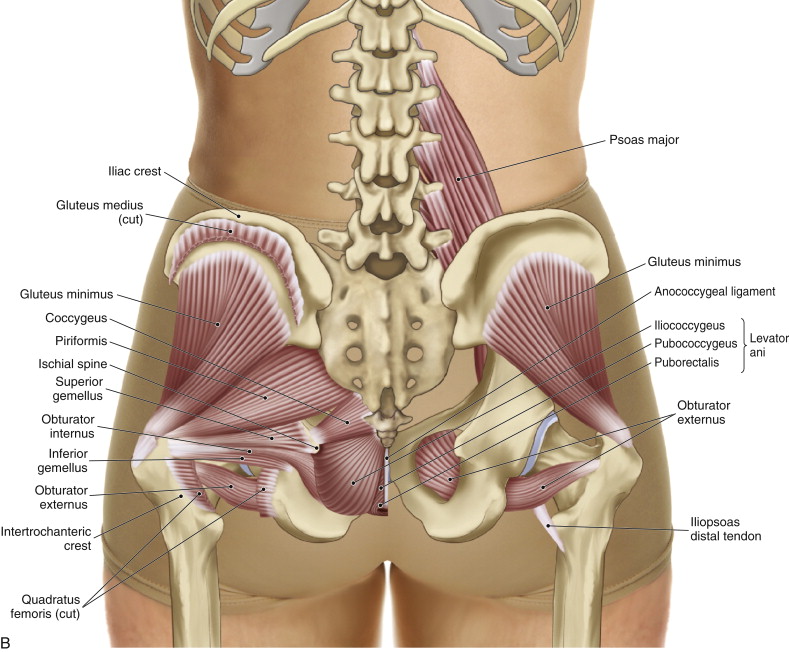
The coccygeus and levator ani are pelvic floor muscles located between the sacrum and coccyx medially and the pelvic bone laterally (Figure 11). As pelvic floor muscles, they are important toward maintaining the stability of the abdominopelvic cavity, and therefore the core of the body. But what it often overlooked is that via their attachments onto the sacrum and coccyx, they can also function to stabilize the sacroiliac joint. The coccygeus specifically attaches from the sacrum (and coccyx) to the pelvic bone, and therefore directly affects sacroiliac function. For this reason, the coccygeus and levator ani should be assessed in every client who presents with sacroiliac pain or dysfunction.
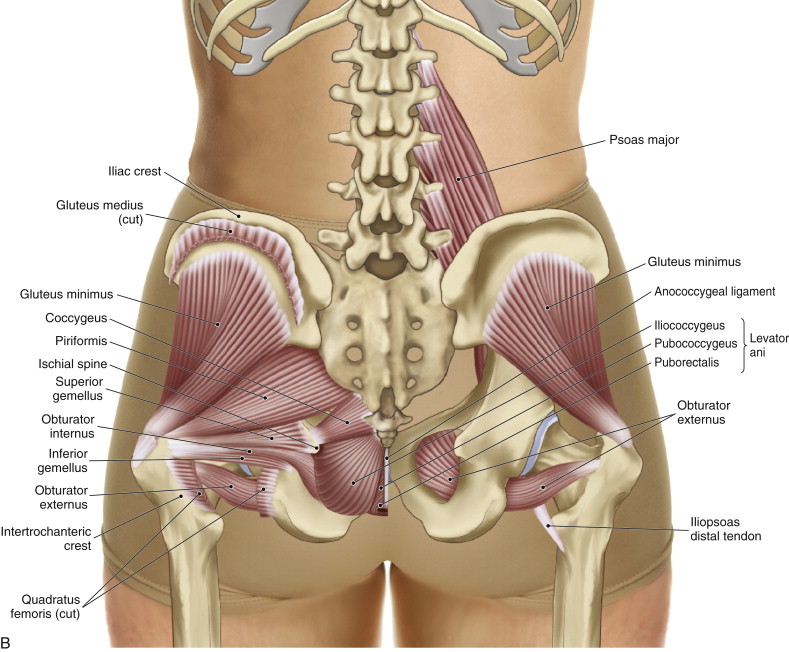
Figure 11. Posterior view of the coccygeus and levator ani. Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
Palpation Assessment of the Coccygeus and Levator Ani
The coccygeus and levator ani are located fairly deep but can usually be easily palpated. Two methods can be used to palpate these muscles. One method is to first locate the coccygeus by locating the piriformis and then dropping inferiorly, maintaining pressure against the sacrum, until the coccygeus is reached. Once the coccygeus has been found, palpate inferior to it for the levator ani. The other method is to instead first locate the levator ani by following from the inferior aspect of the ischial tuberosity to its medial side, then dropping immediately medial to its medial border onto the levator ani. From there, palpate superior to the levator ani for the coccygeus, always hugging close against the coccyx and then sacrum. It is not easy to ask the client to engage these muscles, so they are usually palpated while at rest. Once located, they are assessed.
When palpating these muscles, it is important to be aware of two prominent ligaments located superficially. They are the sacrotuberous and sacrospinous ligaments (Figure 12). The coccygeus can be discerned from the sacrotuberous ligament by noting the different directions of their fibers. It is essentially not possible to discern the coccygeus from the sacrospinous ligament. They run in an identical direction and attach into each other. For this reason, they can be considered to be one myofascial unit.
Note: Many therapists are hesitant to palpate and work these muscles because of their proximity to the anus. However, their dual function as pelvic floor and sacroiliac joint stabilization muscles makes them extremely valuable musculature that should not be skipped. Certainly, given the concern for modesty, verbal consent should be first attained; and careful draping or working the muscles through draping should be done. Further, they can be worked ipsilaterally or contralaterally, whichever is more comfortable for the client.
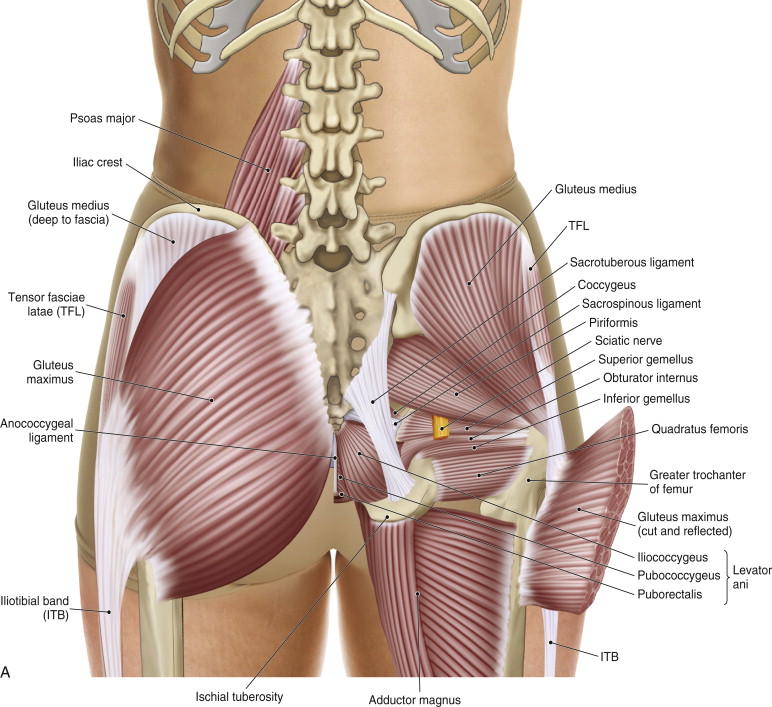
Figure 12. The right sacrotuberous and sacrospinous ligaments. Courtesy of Joseph E. Muscolino. The Muscle and Bone Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. Elsevier 2016.
Stretching the Coccygeus and Levator Ani
It is challenging to stretch the coccygeus and levator ani musculature. If the thigh is abducted, this may place a small force that separates the pelvic bone from the sacrum/coccyx, thereby slightly stretching these muscles.
Case Study – Coccygeus and Levator Ani
Janice was a 35 year-old woman who presented with left gluteal pain. She reported that she had been walking down a staircase and misjudged the number of steps. As a result, she landed hard on her left foot at the bottom of the stairs and felt a jolt of pain shoot up into her left gluteal region. This pain then persisted with each step she took on her left side. She came in for treatment a few days later, complaining of persistent pain near her “tailbone.” During palpation exam, I of course first assessed the piriformis, which was healthy. I then proceeded to assess the quadratus femoris and other deep lateral rotators, but these were also healthy and when pressed did not reproduce any pain or discomfort. As I continued to search for the cause of the pain, Janice kept indicating that her pain was more medial. When I palpated directly lateral to the coccyx, I clearly felt a trigger point that when palpated reproduced her characteristic pain pattern. Four treatments of moist heat and deep massage were successful at resolving her condition.
Note: This blog post article is the fifth in a series of 8 posts on
Unusual Suspect Muscles of the Body*
The 8 Blog Posts in this Series are:
- Introduction
- Palmar Interossei (PI)
- Flexor Pollicis Longus (FPL)
- Quadratus Femoris (QF)
- Coccygeus & Levator Ani
- Sternohyoid
- Longus Colli & Longus Capitis
- Other Unusual Suspects…
* This series of blog post articles is modified from an article originally published in massage and bodywork (m&b) magazine: The Unusual Suspects. November/December 2016 issue.
