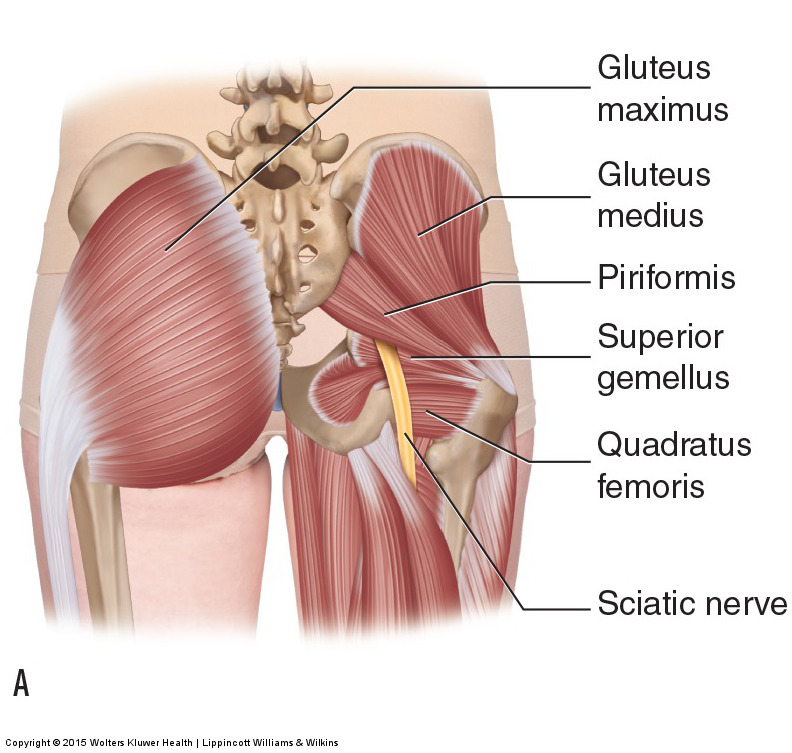

Usual course of the sciatic nerve relative to the piriformis muscle. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Piriformis syndrome is a condition in which a tight piriformis muscle compresses against the sciatic nerve, causing symptoms of sciatica into the lower extremity. The sciatic nerve usually exits from the internal pelvic cavity into the buttock/gluteal region between the piriformis and the superior gemellus muscles. However, in approximately 15% of individuals, part or all of the sciatic nerve passes through the piriformis muscle or above it (between the piriformis and gluteus medius). Regardless of the presentation of the sciatic nerve in the gluteal region, if the piriformis is tight, it can compress against the sciatic nerve and cause piriformis syndrome.
Causes:
In anatomic position, the piriformis is a lateral (external) rotator of the thigh at the hip joint, as well as a contralateral rotator of the pelvis at the hip joint. If the thigh is flexed to approximately 60 degrees or more, the piriformis switches from being a lateral rotator to being a medial (an internal) rotator of the thigh, and also becomes a horizontal abductor of the thigh at the hip joint
. The piriformis also crosses the sacroiliac joint (SIJ) and is therefore active as a stabilizer of the SIJ. Because piriformis syndrome is caused by a tight piriformis muscle, any posture or movement pattern that places a demand on the piriformis to contract can increases the baseline tone of the muscle and cause or contribute to piriformis syndrome.
One of the principal causes of a tight piriformis muscle is when it tightens to stabilize a dysfunctional or painful SIJ. Dysfunctional SIJ conditions include sprain, hypomobility, hypermobility, or a macrotrauma or repeated microtrauma that causes irritation/inflammation and therefore pain at the joint. Of these, pain and hypermobility would most likely cause the piriformis to tighten. The piriformis will also tend to tighten if the client/patient has a chronic posture of lateral rotation of the thigh, thereby allowing the piriformis to adaptively shorten and become tight. This can occur due to driving when the foot is on the gas pedal but the heel is placed in front of the brake; it can also occur in clients who have a habitual pattern of crossing the legs so that the ankle is on the opposite-side knee.
