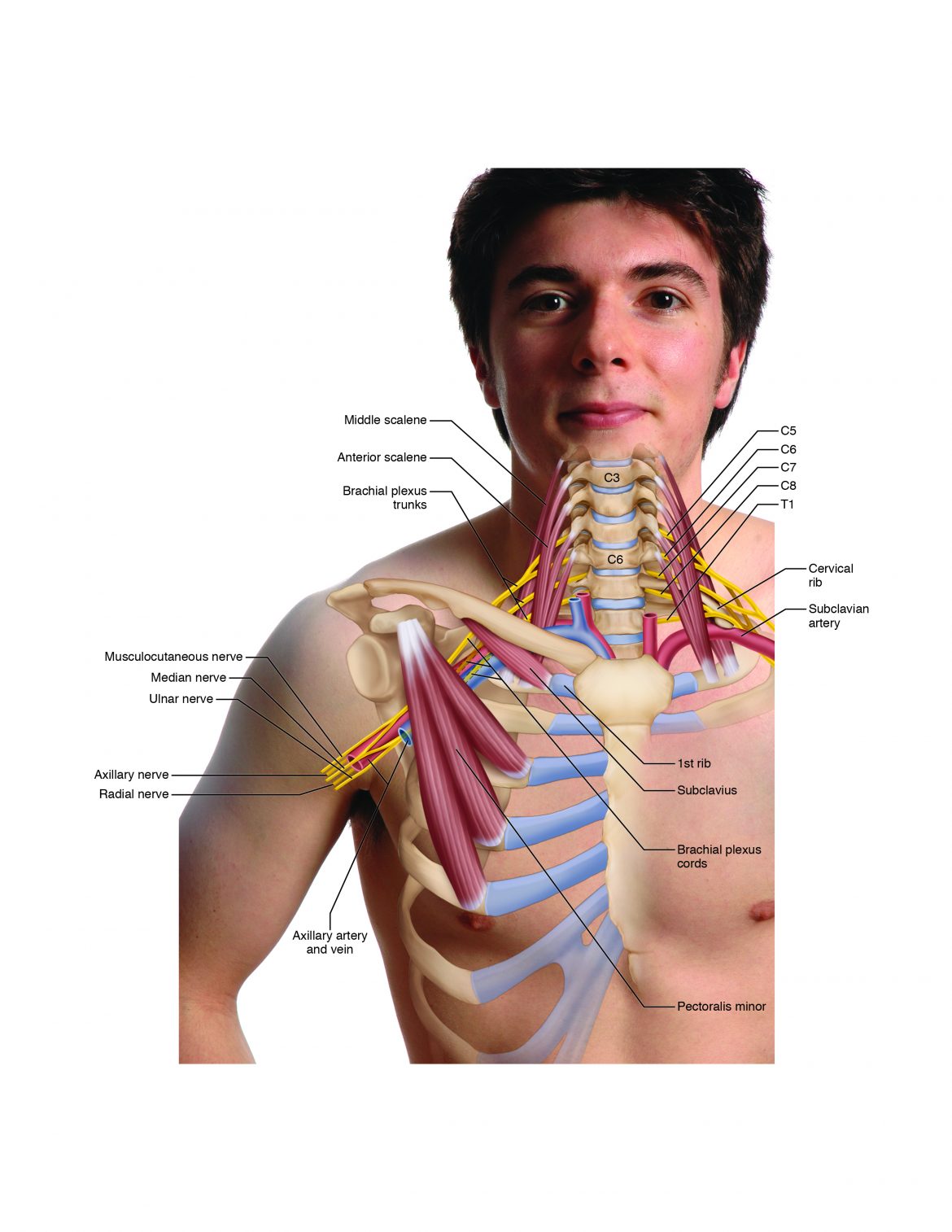
Thoracic outlet syndrome (TOS) is a condition that causes compression of the brachial plexus and/or the subclavian/axillary artery and vein blood vessels where the thorax outlets into the upper extremity. This region is located in the lower neck/chest/axillary area (Fig. 18).
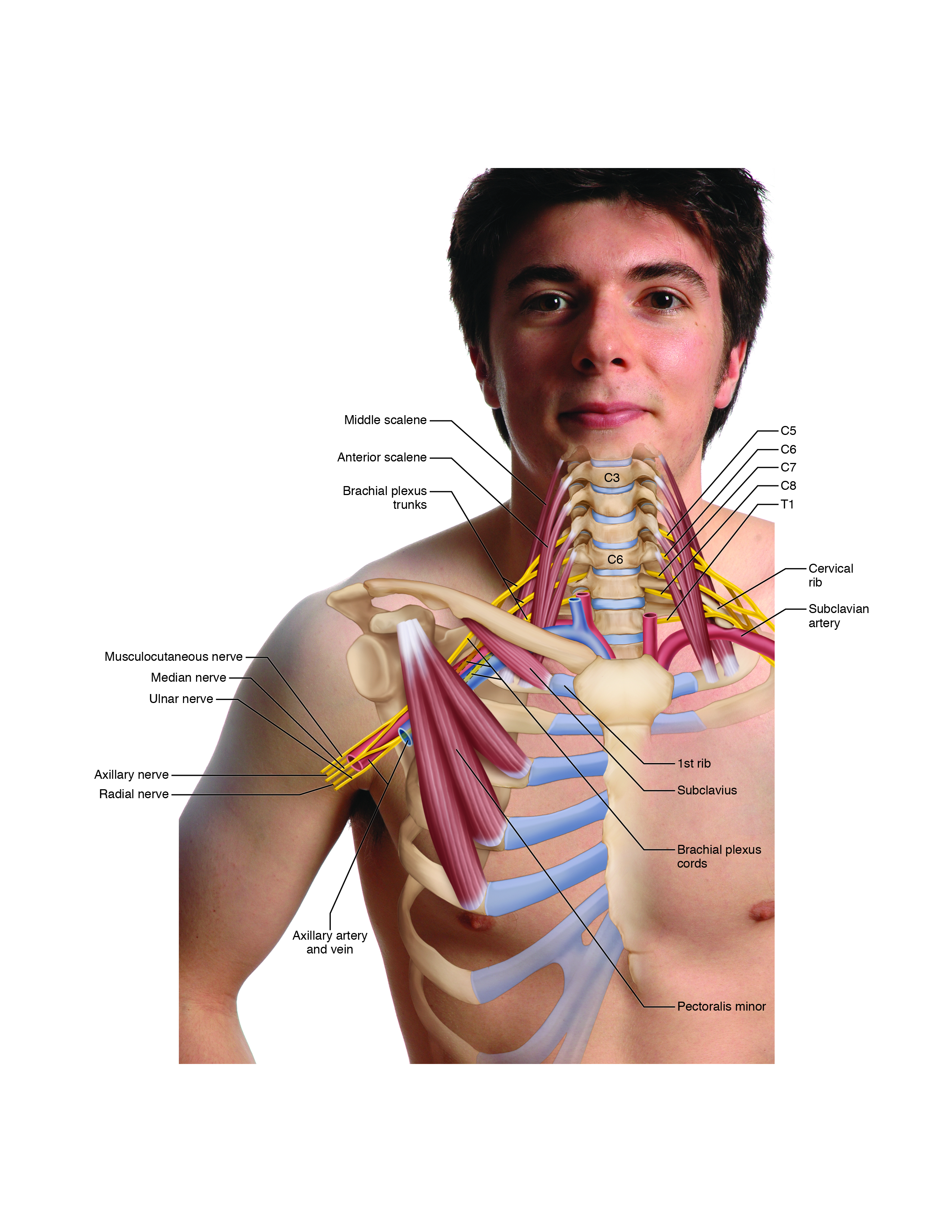
Figure 18. There are four forms of thoracic outlet syndrome (TOS): anterior scalene syndrome, costoclavicular syndrome, pectoralis minor syndrome, and cervical rib syndrome. Figure courtesy of Joseph E. Muscolino DC. Art work by Giovanni Rimasti.
Why Outlet?
This region is considered to be an “outlet” because arteries carry blood out of the thorax and into the arm to nourish the tissues of the upper extremity, and motor neurons carry motor innervation out of the thorax and into the arm to control contraction of the muscles of the upper extremity. However, this condition is sometimes called thoracic “inlet” syndrome because this region is where veins carry blood and sensory neurons carry sensory innervation into the thorax from the arm. Usually, the name TOS is used for any compression in this region, regardless of whether compressed structures are exiting or entering.
Description of Thoracic Outlet Syndrome (TOS)
There are four major types of TOS, each one named for the location of the neurovascular compression:
- Anterior scalene syndrome
- Costoclavicular syndrome
- Pectoralis minor syndrome
- Cervical rib syndrome
All four syndromes involve compression of the brachial plexus and/or the subclavian artery or vein. When sensory neurons of the brachial plexus are involved, the client may experience sensory symptoms such as pain, tingling, or numbness in the arm, forearm, or hand. When motor neurons of the brachial plexus are involved, the client may experience motor symptoms such as weakness of musculature in the arm, forearm, or hand. When arterial supply is compromised because the subclavian artery is compressed, the client may experience a decrease of arterial circulation in the arm, forearm, or hand. In clients with light skin, this will often show as a more bluish hue instead of the normal reddish hue of the skin of the hand. When venous supply is compromised because the subclavian vein is compressed, the client may experience a decrease or loss of venous return of circulation from the hand, forearm, or arm; this will often present as a swelling in the hand. By far, the most commonly affected structures in TOS are the brachial plexus of nerves.
Thoracic Outlet Syndromes Displayed on Poster
Orthopedic Assessment of Thoracic Outlet Syndrome
Understanding Thoracic Outlet Syndromes
Freedom from Thoracic Outlet Syndrome
Assessing Thoracic Outlet Syndrome (TOS)
TOS can cause symptoms in the upper extremity that are similar to those caused by a pathologic cervical disc or cervical DJD. Because treatment should always be directed not at a set of symptoms but at the mechanism that causes them, it is important to assess the underlying cause. Once the condition has been assessed, an appropriate treatment strategy can be determined. Anterior scalene syndrome is assessed with Adson’s test (Fig. 19A). Costoclavicular syndrome is assessed with Eden’s test (also known as military brace position/test) (Fig. 19B). And pectoralis minor syndrome is assessed with Wrights’s test (Note: There are two forms of Wright’s test seen in Figures 20A and 20B).
For Adson’s, Eden’s, and Wright’s, the test is considered positive if the strength of the radial pulse diminishes and/or if the client reports paresthesia symptoms into the upper extremity.
When a cervical rib is present (a genetic anomaly found in approximately 1 in 100 people) causing TOS, Adson’s test will usually show positive. Definitive assessment/diagnosis of a cervical rib is done by X-ray.


Figure 19. A, Adson’s test for anterior scalene syndrome. B, Eden’s test for costoclavicular syndrome.
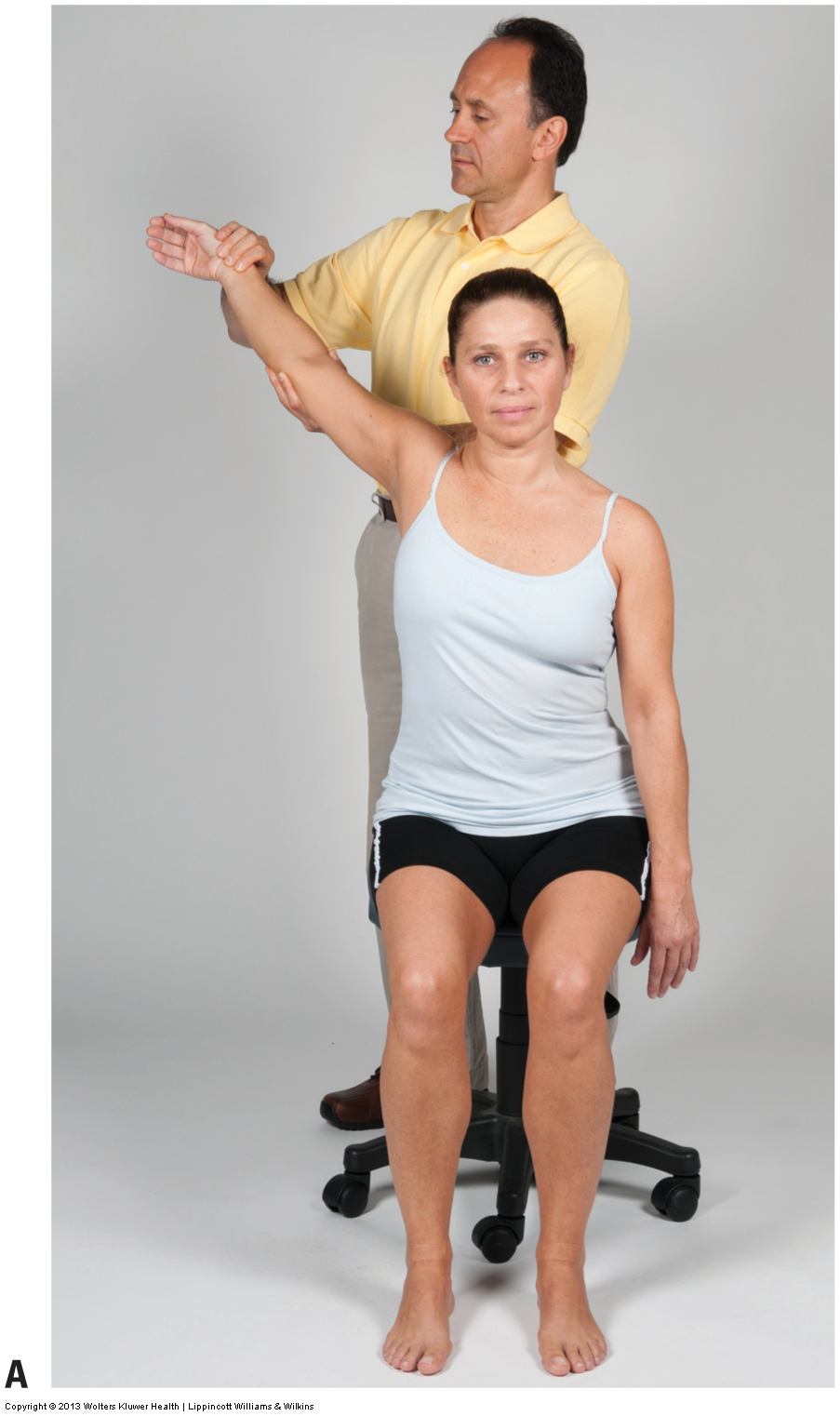
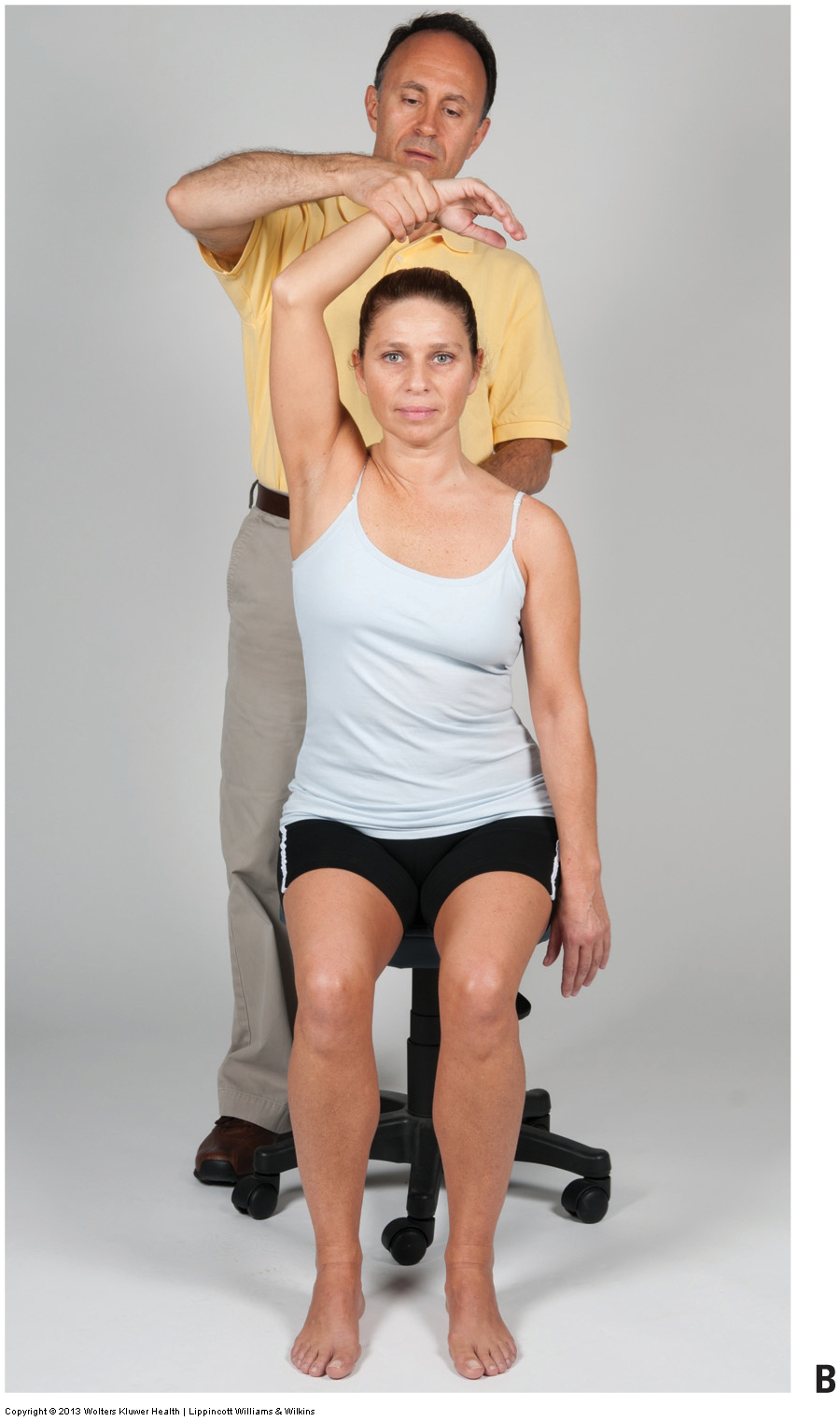
Figure 20. Wright’s tests for pectoralis minor syndrome. A, Version 1. B, Version 2.
Mechanism and Causes of Thoracic Outlet Syndrome:
Anterior Scalene Syndrome
Anterior scalene syndrome involves compression between the anterior and middle scalene muscles. Compression occurs if the scalene muscles become tight and squeeze the neurovascular structures located between them. Scalenes often become tight as a result of a whiplash accident or prolonged shortening that occurs from a forward head posture.
Costoclavicular Syndrome
Costoclavicular syndrome involves compression between the clavicle and first rib, the region known as the costoclavicular space. Costoclavicular syndrome results from poor posture known as the upper crossed syndrome, in which the client’s upper trunk/spine rounds forward and down into flexion, the shoulder girdles round forward into protraction, and the arms medially/internally rotate at the glenohumeral joints (note: upper crossed syndrome usually results in dueling locked short – locked long opposing groups of musculature). This posture is usually the result of tight scapular protractors (pectoralis major and minor), weakened scapular retractors (rhomboids and trapezius, especially the middle trapezius), and weakened upper back extensors (erector spinae and semispinalis). This posture causes the clavicle to fall forward and down against the first rib, closing down on the costoclavicular space and compressing the neurovascular structures located there. Costoclavicular syndrome may also occur if the subclavius, anterior scalene, and/or middle scalene muscles become tight and pull the first rib up against the clavicle. Another factor that can cause or contribute to this condition is a bony callus on the clavicle secondary to its having been fractured.
Pectoralis Minor Syndrome
Pectoralis minor syndrome involves compression between the pectoralis minor and the ribcage. This occurs because of a tight pectoralis minor that compresses the neurovascular structures between it and the ribcage. A tight and shortened pectoralis minor also causes the rounded scapular protraction posture mentioned previously in the explanation of the costoclavicular syndrome. Weakened scapular retractors contribute to this posture by lacking the strength to counter the pull of the tight pectoralis musculature.
Cervical Rib Syndrome
The presence of an anatomic anomaly called a cervical rib can also cause neurovascular compression characteristic of TOS. A cervical rib is usually a small bone that forms off of C7. Its location may cause impingement on the brachial plexus, usually between the anterior and middle scalenes. Cervical ribs occur in approximately 1% of the population.
Note: Treatment Considerations in Brief for Thoracic Outlet Syndrome
Massage and stretching can be extremely beneficial in helping to decrease muscular tightness and spasms associated with TOS. When working the anterior neck for anterior scalene syndrome, there are precautions and contraindications to consider given the number of sensitive structures present.
Moist heat before stretching is also valuable. Strengthening the extensors of the thoracic spine and retractors of the shoulder girdles is also extremely important.
(Note: For more on the Thoracic Spine, click here.)
Note: This blog post article is the seventh in a series of 10 posts on
Common Musculoskeletal* Conditions of the Neck
The 10 Blog Posts in this Series are:
- Fascial Adhesions (and an introduction to musculoskeletal conditions of the neck)
- Hypertonic (tight) musculature
- Joint dysfunction
- Sprains and strains
- Pathologic disc conditions
- Osteoarthritis (OA)
- Thoracic outlet syndrome (TOS)
- Forward head posture
- Tension headaches
- Greater occipital neuralgia
(*perhaps a better term is “neuro-myo-fascio-skeletal”)
