Causes of spinal joint dysfunction
Hypomobility
A hypomobility is a joint whose motion is restricted. Therefore any factor that can limit motion at the joint can cause or contribute to a hypomobility. The primary causes of spinal joint hypomobility can be divided into three types: taut soft tissue, bony obstruction, and jammed meniscoid body.
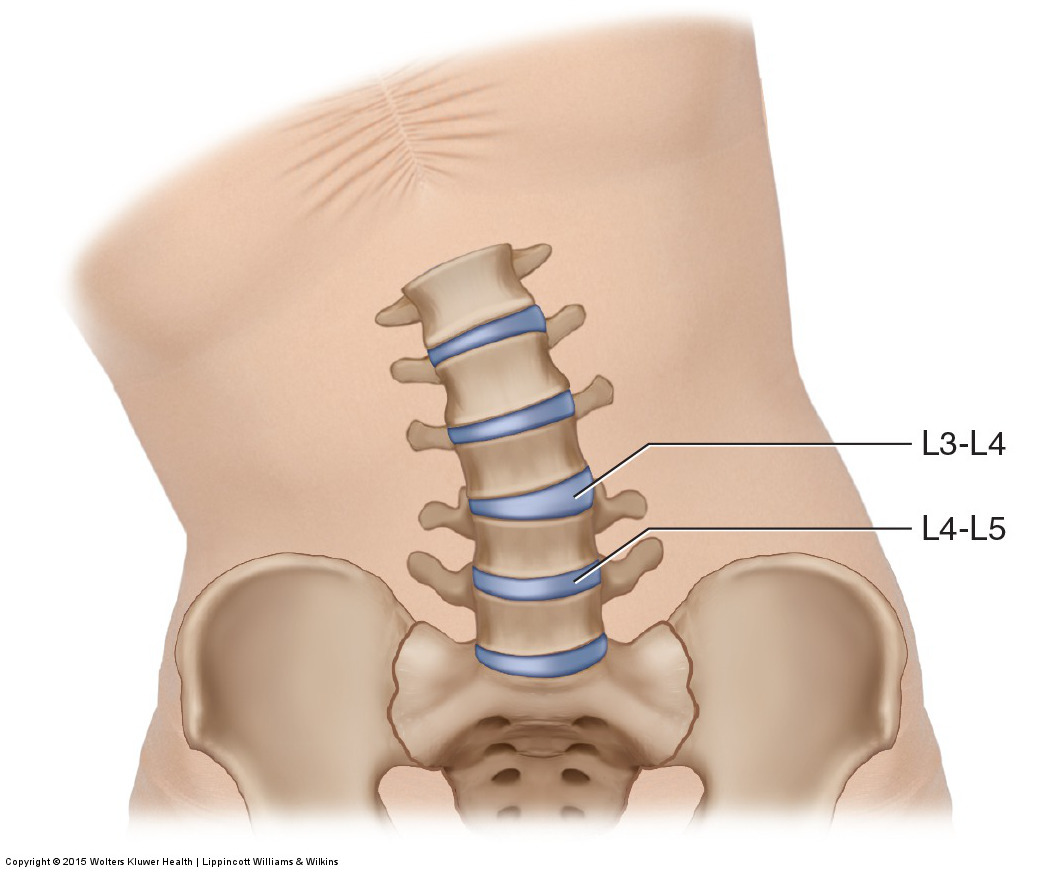
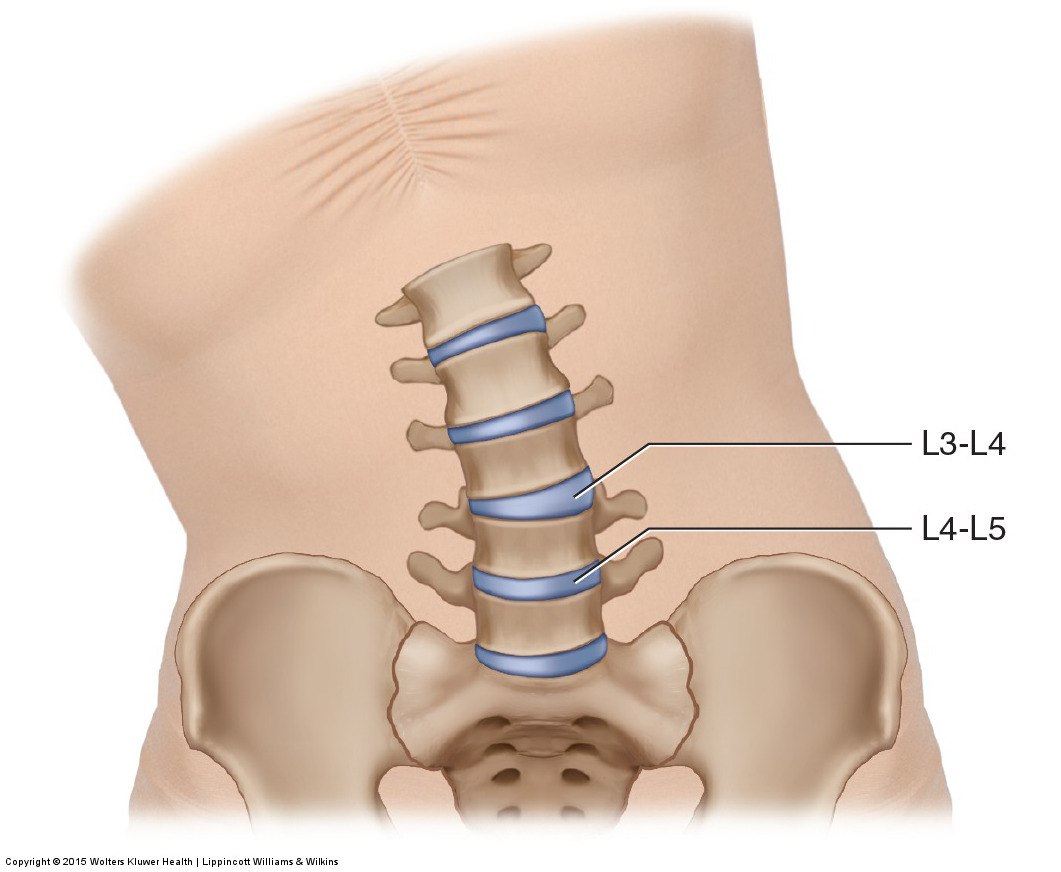
A hypomobile joint dysfunction at L4-L5 creates a hypermobile joint dysfunction at L3-L4. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
One major cause of soft tissue restriction is tight/hypertonic musculature, whether it is global tightening of the muscle or a myofascial trigger point. Muscle tightness can occur due to irritation/injury to the muscle itself, a muscle spindle stretch reflex, or muscle tightening via the pain-spasm-pain cycle to splint and protect an injury in the area. Because of the large number of joints in the spine and the tremendous demand upon the spine for motion, muscle contraction for stabilization is particularly important, and when excessive can result in hypomobile joints. Although every tight muscle can restrict motion, it is often the smaller deeper postural muscles of the spine that tighten to cause joint hypomobility. These muscles are the rotatores, multifidus, and semispinalis of the transversospinalis group, as well as the interspinales and intertransversarii. Muscle tautness can also occur due to the presence of fascial adhesions (“fuzz” in the parlance of Gil Hedley) within the muscle or between planes of muscles.
The other major cause of soft tissue restriction is taut fascial tissues. These include spinal ligaments, facet joint capsules, and other fascial membranes (such as the thoracolumbar fascia). Taut fascial tissue can occur from lack of motion as well as a buildup of fascial adhesions.
The most common bony cause of hypomobility involves the presence of degenerative osteoarthritic bone spurs located at a joint margin that can block motion of the bones at the joint. These degenerative changes are the body’s response (known as Wolff’s Law) to excessive physical stress placed upon the joint surfaces. These bone spurs may form along the surfaces of the facet joints or along the margins of the vertebral bodies. Most of the time, bone spurs are not large enough to actually interfere with joint motion. However, when advanced, they can contribute to a hypomobile joint.
Note: Osteoarthritis of the spine is given a special name: spondylosis (not to be confused with the term/condition: spondylolisthesis).
Other conditions of bone tissue can also be the cause of bony obstruction of movement. These include abnormal curvatures of the spine such as scolioses, hyperlordotic, and hyperkyphotic curves because these conditions can cause jamming of the facets when motion is attempted. A surgical spinal fusion is an additional cause of joint hypomobility in the spine.
Taut soft tissues and bony obstruction can be factors in all joint dysfunction hypomobilities of the body. However, in the case of spinal joints, a third cause of hypomobility has been proposed; that is a meniscoid body that has become pinched and jammed between the surfaces of the facet joint. A meniscoid body is a fibrous, fatty soft tissue that is located at the periphery of a joint space. If it displaces and moves toward the center of the joint, it can become pinched and swollen, obstructing motion toward that side of the joint.
In addition to these primary causes of joint hypomobility, a common secondary cause of hypomobile spinal joints is overuse due to compensatory hypermobility. When one segmental joint level is hypomobile, the adjacent joint will often become hypermobile to compensate so that the region still has full gross range of motion. In time, excessive motion at the compensatory hypermobile joint level can lead to overuse and irritation to that joint (in the parlance of Leon Chaitow: “used, overused, misused, abused”), thereby triggering muscle tightness to splint and stop its motion. Now there are two segmental hypomobile joints, causing the next adjacent joint level to become even more hypermobile to compensate. In time, this second hypermobility can also become overused and irritated, triggering muscle tightness and causing it to become hypomobile. In this manner, hypomobilities often spread through the spine. Because the musculature that tightens is often small intrinsic musculature, this condition is usually not symptomatic until the region of hypomobility is so great that full compensation by adjacent joints is not possible and gross range of motion decreases.
The longer a hypomobile joint or hypomobile region is allowed to exist, the worse it becomes. Lack of motion allows for the continued deposition of fascial adhesions that increasingly lock up the area. Allowing a hypomobility to continue also allows the increased muscle tone of the region to become more patterned into the nervous system. For these reasons, joint hypomobility tends to be a progressive condition that expands in both intensity and in scope throughout the spine. Indeed, it is not uncommon for middle aged and elderly clients to have large regions of their spine locked in hypomobility. The over all result is that once begun, this pattern of hypomobility progressively worsens as we age.
Hypermobility
There are generally three major causes of hypermobile joint dysfunction in the spine. The first is an injury that causes a sprain of spinal ligaments and joint capsules. The best example is a whiplash. The second cause is when the client/patient engages excessively in an activity that gradually over time (over)stretches the fascial tissues of the spine. Examples are yoga and gymnastics. Once fascial ligament/joint capsules are torn or overstretched, whether it is by injury or choice, they usually remain unstable forever. This results in hypermobile instability at the joints affected. The third cause of hypermobility in the spine is when a spinal joint is moved more as a compensation for nearby hypomobile segments as previously discussed.
