Iliotibial Band Syndrome
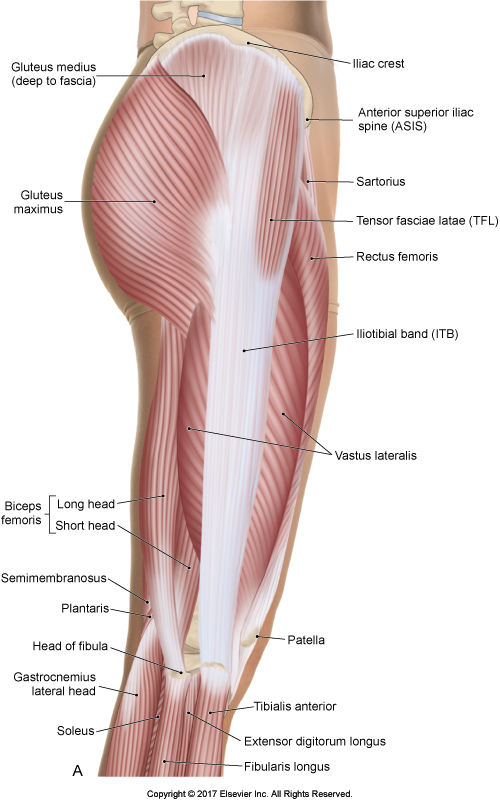
Iliotibial Band. Permission Joseph E. Muscolino. The Muscular System Manual – The Skeletal Muscles of the Human Body, 4th ed. (Elsevier 2017).
Iliotibial Band Syndrome has been associated with altered hip and knee kinematics in runners. There has been a suggestion that neuromuscular factors at the hip may play an important role in iliotibial band syndrome syndrome.
Comment by Joseph Muscolino
Iliotibial band syndrome is not simply pain or tightness in the lateral thigh over the iliotibial band. In fact, pain and tightness in the lateral thigh is often due to tightness of the underlying vastus lateralis and vastus intermedius of the quadriceps femoris group, and not the more superficial iliotibial band. Rather, iliotibial band syndrome is a friction syndrome that occurs when the iliotibial band rubs over the lateral femoral condyle with repeated flexion and extension of the knee joint, as occurs so often with running and cycling.
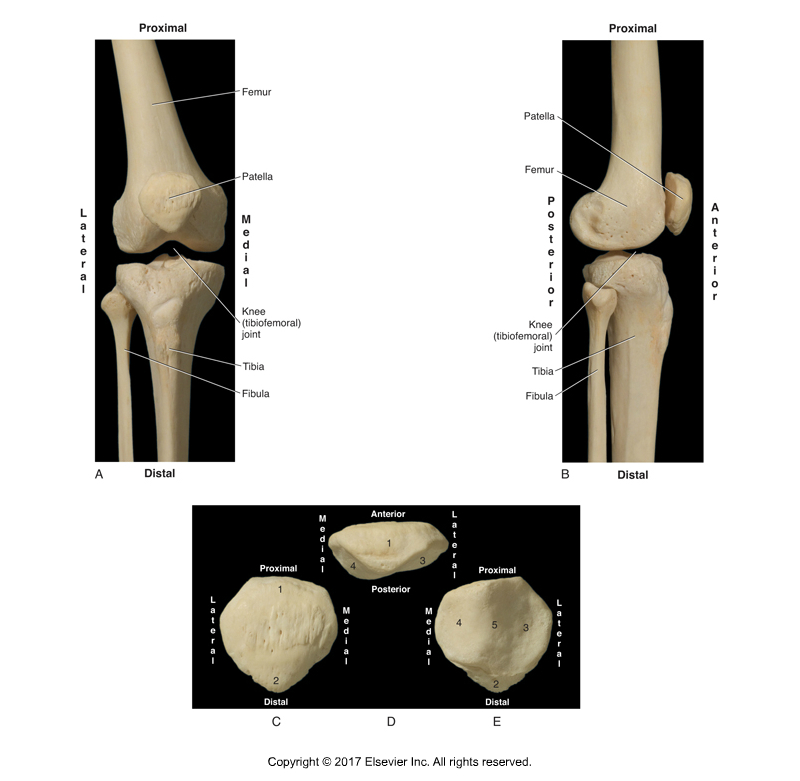
The right knee joint, anterior and lateral views; and the patella. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. (Elsevier, 2017).
Study
A study compared hip surface electromyography, and frontal plane hip and knee kinematics, in runners with and without iliotibial band syndrome.
The study was an observational cross-sectional study. Thirty subjects were recruited consisting of 15 injured runners with iliotibial band syndrome and 15 gender, age and body mass index matched controls. In each group, eight were male runners and seven were female runners. Inclusion criteria for the injured group were pain within two months related to iliotibial band syndrome and a positive Noble compression test.
Motion Capture
 Three-dimensional motion capture was performed using ten high speed cameras synchronized with wireless surface electromyography during a 30-minute run. The first data point was at three minutes using a constant speed of 2.74 meters per second. A second data point was at 30 minutes using a self-selected pace by the participant to allow for a challenging run until completion at 30 minutes.
Three-dimensional motion capture was performed using ten high speed cameras synchronized with wireless surface electromyography during a 30-minute run. The first data point was at three minutes using a constant speed of 2.74 meters per second. A second data point was at 30 minutes using a self-selected pace by the participant to allow for a challenging run until completion at 30 minutes.
Motion capture was reported as peak kinematic values from heel strike to peak knee flexion for hip adduction and knee adduction (genu varum – bow leg – See Figure B below). Surface electromyography was reported as a percentage of maximal voluntary contraction for the gluteus maximus, gluteus medius, and tensor fascia latae muscles.
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s video streaming subscription service for manual and movement therapists, has an entire folder of video lessons on pathomechanics of common musculoskeletal conditions? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
Results

Excessive genu valgum and genu varum. Knee adduction (genu varum) is shown in Figure B. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. (Elsevier, 2017).
The data showed that injured runners showed increased knee adduction compared to control runners at 30 minutes (control = -1.48°, injured = 3.74°). Tensor fasciae latae muscle activation in injured runners was increased compared to control runners at three minutes (control = 7% MVIC, Injured = 11% MVIC).
Conclusion
The authors suggested that lateral knee pain in runners localized to the distal iliotibial band is associated with increased knee adduction at 30 minutes. Increased Tensor Fasciae Latae (TFL) muscle activation at three minutes is noted but more investigation is needed to better understand the clinical meaning. These findings are consistent with but not conclusive evidence supporting the theory that neuromuscular factors of the hip muscles may contribute to increased knee adduction in runners with iliotibial band syndrome.
Nevertheless, the authors advise caution using these findings to support treatments intended to modify TFL activation given the small differences of four percent in muscle activation. Increased knee adduction in runners at 30 minutes was over five degrees and beyond the minimal detectable difference. Additional research is needed to confirm if the degree of knee adduction changes earlier versus later in a run, and whether or not fatigue is a clinically relevant factor.
Comment by Joseph E. Muscolino
This study seems to show a relationship between iliotibial band (ITB) syndrome and knee adduction (genu varum). It also seems to show a relationship between activation of certain hip joint musculature (TFL) and these two conditions. A relationship can be two incidents that occur together, termed a “coincidence.” Or there can be a causal relationship between them; i.e., one causes the other to occur. In this case, looking at the relationship of iliotibial band syndrome and knee adduction (genu varum), the question might be: does ITB syndrome cause knee adduction or does knee adduction cause ITB syndrome, or both?
It would seem to make sense that the postural distortion pattern of knee adduction would stretch out the ITB across the lateral thigh and knee, causing it to be more taut, and therefore rub with greater friction against the lateral condyle of the femur. So it would seem that knee adduction would be a predisposing factor toward developing ITB syndrome. Does ITB syndrome cause knee adduction? Well, ITB syndrome would seem to more likely occur when the ITB is taut. And this would occur if either the TFL or the gluteus maximus were tight. And when these muscles, which are hip abductors, are tight, they might predispose the femur to be in slightly greater abduction, which would then predispose the tibias to angle in more medially toward a normal stance of the feet, thereby creating knee adduction. And certainly, we would also now have a causal relationship between the increased tone of the TFL and the ITB syndrome and knee adduction. Please keep in mind that this is an extrapolation of “predisposing” factors mechanically. Further research study might bear this out. But it does make sense mechanically.
This blog post article was created in collaboration with www.terrarosa.com.au.
(Click here for the blog post article: What is iliotibial band syndrome and what are its causes?)
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s video streaming subscription service for manual and movement therapists, has an entire folder of video lessons on pathomechanics of common musculoskeletal conditions? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
