Introduction
Golfer’s elbow (medial epicondylitis/epicondylosis) is assessed through active and passive wrist range of motion testing, manual resistance, palpation of the medial epicondyle, and — when needed — diagnostic imaging such as ultrasound or MRI. Whether you’re a massage therapist, physical therapist, chiropractor, or sports medicine clinician, a systematic assessment approach is the difference between accurate diagnosis and a missed or mismanaged condition.
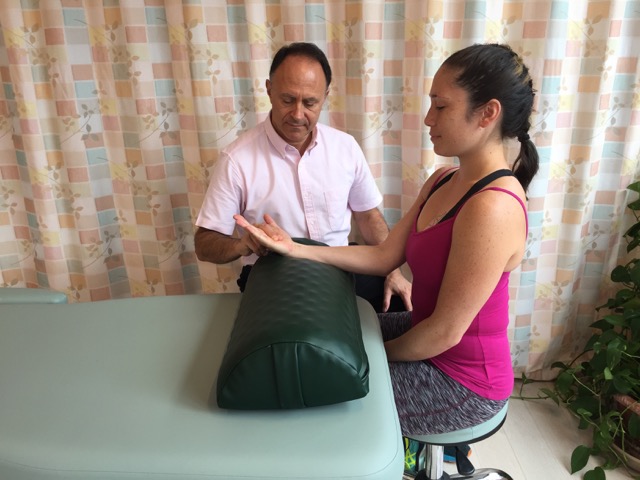
Manual resistance to flexion of the hand at the wrist joint will cause pain (show positive) for a client/patient with golfer’s elbow. Permission: Joseph E. Muscolino.
Medial elbow pain is far more common than its name suggests — you don’t need to swing a golf club to develop it. Repetitive gripping, lifting, and forearm flexor overload in jobs ranging from carpentry to desk work can trigger it. This guide gives you a complete, clinically grounded framework for identifying golfer’s elbow and ruling out conditions that mimic it.
What Exactly Is Golfer’s Elbow — and Why Does Assessment Matter?
Golfer’s elbow is a degenerative or inflammatory condition of the common flexor tendon at its attachment to the medial epicondyle of the humerus. Accurate assessment matters because medial elbow pain has several mimics — including cubital tunnel syndrome and medial collateral ligament injury — and misdiagnosis leads to ineffective treatment.
The condition is clinically termed medial epicondylitis (when acute/inflammatory) or medial epicondylosis (when chronic/degenerative). Research consistently shows that chronic presentations are predominantly degenerative rather than inflammatory, a distinction that shapes the entire treatment approach.
Key anatomy involved:
- Common flexor tendon — origin of the wrist and finger flexors (flexor carpi radialis, palmaris longus, flexor carpi ulnaris, flexor digitorum superficialis, and pronator teres)
- Medial epicondyle of the humerus — the bony attachment point
- Ulnar nerve — runs close to the medial epicondyle and may be involved in up to 20–30% of cases (Gabel & Morrey, 1995)
Original Clinical Insight #1: In the authors’ experience teaching manual therapy practitioners, golfer’s elbow is consistently underdiagnosed relative to tennis elbow — partly because patients and clinicians alike anchor on the better-known lateral presentation. Practitioners who routinely screen the medial epicondyle during any forearm complaint catch it earlier.
How Do You Perform Active Range of Motion Tests for Golfer’s Elbow?
Active range of motion (AROM) of the wrist and fingers is the first line of functional assessment. Pain reproduced during active wrist flexion or finger flexion strongly implicates the common flexor tendon and its medial epicondyle attachment.
When you ask your patient to actively flex the hand at the wrist or curl the fingers at the MCP and PIP joints, the flexor musculature contracts concentrically, generating tension at its proximal tendon. If that tendon is irritated or degenerated, pain is reproduced at the medial elbow — a positive finding.
AROM Test Protocol:
- Position the patient seated with the elbow at approximately 90° flexion, forearm in supination, resting on a table.
- Ask the patient to actively flex the wrist — watch for pain at the medial epicondyle region.
- Ask the patient to actively flex the fingers — same observation applies.
- Then ask for active wrist extension — this eccentrically loads and stretches the flexors, also frequently positive.
- Test radial and ulnar deviation — either or both may be painful depending on which muscles are most involved.
What the findings mean:
| Motion Tested | Expected Finding in Golfer’s Elbow | Why |
|---|---|---|
| Active wrist flexion | Painful (positive) | Concentric flexor contraction at medial epicondyle |
| Active finger flexion | Painful (positive) | Same mechanism via FDS attachment |
| Active wrist extension | Painful (positive) | Eccentric stretch on the common flexor tendon |
| Passive wrist extension | Painful (positive) | Stretches flexors without their contraction |
| Passive wrist flexion | Often pain-free | No tensile load on the tendon |
| Ulnar/radial deviation | Variable | Depends on ulnar deviator involvement |
How Does Passive Range of Motion Testing Help Diagnose Golfer’s Elbow?
Passive range of motion (PROM) testing isolates the mechanical (tensile) component from the contractile component. Passive wrist or finger extension is typically positive in golfer’s elbow because it stretches the common flexor tendon without requiring muscular contraction.
This is a critical distinction. If AROM is positive but PROM is negative, you may be dealing with a purely contractile lesion — a muscle tear or significant trigger point activity — rather than a tendinopathy at the epicondyle.
In golfer’s elbow, passive wrist extension and passive finger extension elongate the wrist and finger flexors, placing tensile stress on the common flexor tendon’s medial epicondyle attachment. This reproduces the characteristic deep, aching pain — and sometimes a sharp twinge — at the medial elbow.
Clinical Pearl: Always compare bilaterally. Due to occupational or sport-related asymmetry, the symptomatic side may show noticeably reduced pain-free end-range compared to the asymptomatic side.
What Is the Manual Resistance Test for Golfer’s Elbow?
Manual resistance testing (resisted isometric contraction) is one of the most reliable clinical tests for golfer’s elbow. Resisting wrist flexion or finger flexion with the elbow extended reproduces pain at the medial epicondyle in positive cases.
This is often considered the gold-standard orthopedic assessment maneuver for the condition. By applying manual resistance to the patient’s wrist flexion while keeping the joint stationary, you isolate the contractile stress on the tendon without producing joint motion — which helps rule in a tendon problem rather than a joint problem.
How to perform the resisted wrist flexion test:
- Seat the patient with the forearm in supination, wrist in neutral.
- Stabilize the forearm proximal to the wrist with one hand.
- Apply resistance to the palm, asking the patient to flex the wrist against your resistance — no movement should occur (isometric).
- A positive test = reproduction of medial elbow pain.
- Repeat with resistance applied to finger flexion.
A 2019 systematic review in the Journal of Hand Surgery found that resisted wrist flexion and resisted middle finger flexion had sensitivities of approximately 72–89% for medial epicondylitis when combined with medial epicondyle palpation tenderness.
Original Clinical Insight #2: Practitioners often stop at wrist flexion resistance and miss finger flexor involvement. Testing resistance to individual finger flexion — particularly the ring and middle fingers via FDS — can reveal involvement that wrist testing alone does not capture. This matters for treatment planning, especially in manual therapy.
How Is Palpation Used to Assess Golfer’s Elbow?
Palpation of the medial epicondyle and the proximal common flexor tendon is essential in any golfer’s elbow assessment. Tenderness directly over or just distal to the medial epicondyle is a hallmark finding.
Palpation provides localization that range of motion and resistance testing cannot. It tells you exactly where the pathology is concentrated — whether at the bony attachment, along the tendon body, or in the muscle belly itself.
Palpation assessment guide:
- Medial epicondyle — firm pressure directly over the bony prominence; marked tenderness is positive for epicondylopathy
- Common flexor tendon (1–2 cm distal to the epicondyle) — tenderness here suggests mid-tendon involvement
- Muscle bellies (proximal forearm) — diffuse tenderness may indicate myofascial trigger point involvement
- Ulnar nerve groove (posterior to medial epicondyle) — tenderness here with tingling/numbness into the ring/little finger suggests concurrent cubital tunnel syndrome, which affects 20–30% of golfer’s elbow patients
Visual inspection note: In more significant or long-standing cases, the normal bony contours of the medial elbow may appear less defined compared to the contralateral side, suggesting swelling or thickening of the soft tissue envelope around the epicondyle.
When Should Imaging Be Used to Diagnose Golfer’s Elbow?
Imaging is not required for the initial clinical diagnosis of golfer’s elbow, but ultrasound and MRI are the most accurate tools when the extent of tendon degeneration or tearing needs to be established — particularly before interventional or surgical decisions.
Most cases of golfer’s elbow are diagnosed clinically. Imaging becomes relevant when:
- Symptoms are severe, prolonged (>3 months), or not responding to conservative care
- You need to rule out partial or complete tendon rupture
- Nerve involvement is suspected (MRI can visualize cubital tunnel pathology)
- The diagnosis is uncertain (atypical pain pattern, suspected MCL injury, stress fracture)
Imaging options compared:
| Modality | Best Use | Limitations |
|---|---|---|
| Ultrasound | Dynamic assessment, tendon thickness, calcifications, real-time guided injection | Operator-dependent; less soft-tissue contrast |
| MRI | Full assessment of tendon, ligament, and nerve; gold standard for surgical planning | Cost, availability, no dynamic assessment |
| X-ray | Rule out bony pathology, calcification | Cannot visualize soft tissue directly |
| Nerve conduction study | Confirm/rule out ulnar nerve involvement | Adds time and cost; necessary when neuropathy suspected |
A 2021 study in Skeletal Radiology demonstrated that high-resolution ultrasound and MRI had comparable accuracy in detecting partial-thickness common flexor tendon tears (sensitivity ~85% and ~88%, respectively), supporting either modality for moderate-to-severe cases.
How Do You Perform a Differential Diagnosis for Golfer’s Elbow?
Differential diagnosis is straightforward in most presentations, but three conditions routinely mimic golfer’s elbow: distal wrist flexor tendinitis, cubital tunnel syndrome, and medial collateral ligament injury. Location of pain and specific provocative tests help distinguish them.
| Condition | Pain Location | Key Differentiating Test |
|---|---|---|
| Golfer’s elbow | Medial epicondyle / proximal forearm | Palpation + resisted wrist flexion positive at medial epicondyle |
| Distal wrist flexor tendinitis | Distal forearm / wrist | Same AROM/resistance pattern, but pain localizes distally near the wrist |
| Cubital tunnel syndrome | Medial elbow + ring/little finger | Tingling/numbness with elbow flexion compression test |
| MCL sprain | Deep medial elbow | Valgus stress test positive; no flexor resistance pain |
| Myofascial trigger points | Diffuse forearm pain ± referral | TrP palpation reproduces referred pain pattern; no epicondyle tenderness |
Original Clinical Insight #3: Myofascial trigger points (TrPs) in the wrist and finger flexors can exist alongside — and can also precede — the development of medial epicondylosis. Clinicians who address TrPs early in the course of forearm flexor overuse may reduce the tensile load on the common flexor tendon and potentially slow the progression toward tendinopathy. This integrated perspective bridges the manual therapy and sports medicine approaches.
What Are the Most Reliable Orthopedic Tests for Golfer’s Elbow?
The most clinically reliable orthopedic tests for golfer’s elbow are: (1) resisted wrist flexion test, (2) resisted finger flexion test, (3) medial epicondyle palpation, and (4) the “golfer’s elbow test” (valgus extension overload combined with wrist flexion). Using at least two positive findings improves diagnostic accuracy.
No single test has perfect specificity or sensitivity. The standard clinical practice is to use a cluster of tests:
Recommended assessment cluster:
- ✅ Active wrist flexion AROM — pain at medial epicondyle
- ✅ Passive wrist extension PROM — pain at medial epicondyle
- ✅ Resisted wrist flexion (isometric) — pain at medial epicondyle
- ✅ Resisted finger flexion (isometric) — pain at medial epicondyle
- ✅ Palpation — direct tenderness at/just distal to medial epicondyle
When three or more of these are positive and pain consistently localizes to the medial epicondyle, a clinical diagnosis of golfer’s elbow is well-supported and conservative treatment can begin.
Golfer’s Elbow vs. Tennis Elbow: How Does the Assessment Differ?
The assessment approach for golfer’s elbow (medial) mirrors that of tennis elbow (lateral), but targets the opposite side of the elbow. Golfer’s elbow involves flexors and the medial epicondyle; tennis elbow involves extensors and the lateral epicondyle.
| Feature | Golfer’s Elbow | Tennis Elbow |
|---|---|---|
| Epicondyle involved | Medial | Lateral |
| Tendon involved | Common flexor tendon | Common extensor tendon |
| AROM that causes pain | Wrist/finger flexion | Wrist/finger extension |
| PROM that causes pain | Wrist/finger extension | Wrist/finger flexion |
| Resisted test positive | Wrist flexion | Wrist extension |
| Nerve at risk | Ulnar nerve | Posterior interosseous nerve (PIN) |
Learn more in our related article: How to Assess (Diagnose) Tennis Elbow
Frequently Asked Questions About Golfer’s Elbow Assessment
What is the best physical test for golfer’s elbow?
The resisted wrist flexion test (isometric contraction against manual resistance with the elbow extended) combined with direct palpation tenderness at the medial epicondyle is considered the most reliable clinical test cluster. Using both together improves diagnostic specificity significantly over either test alone.
Can you diagnose golfer’s elbow without imaging?
Yes. In the majority of cases, golfer’s elbow is diagnosed clinically using range of motion assessment, manual resistance testing, and palpation. Imaging (ultrasound or MRI) is reserved for severe, persistent, or atypical presentations, or when surgical or injection-based interventions are being considered.
How do you tell the difference between golfer’s elbow and cubital tunnel syndrome?
Golfer’s elbow produces pain local to the medial epicondyle and proximal forearm, reproduced by wrist and finger flexion tests. Cubital tunnel syndrome involves ulnar nerve compression at the elbow, producing tingling, numbness, or weakness in the ring and little fingers. The elbow flexion compression test helps identify cubital tunnel syndrome; approximately 20–30% of golfer’s elbow patients have concurrent ulnar nerve involvement.
Where exactly does golfer’s elbow hurt on palpation?
Tenderness is typically at the medial epicondyle itself or within 1–2 cm distal along the common flexor tendon. In more chronic cases, the tendon may feel thickened or nodular. Comparing to the uninvolved side helps identify subtle changes.
Does golfer’s elbow show up on X-ray?
Standard X-ray does not visualize soft tissue and will typically appear normal in golfer’s elbow. It can reveal calcifications within the tendon (uncommon) or bony abnormalities that might suggest an alternative diagnosis. Ultrasound and MRI are the preferred imaging modalities for soft tissue assessment.
Can golfer’s elbow be present without playing golf?
Absolutely. Despite the name, golfer’s elbow affects a wide range of people including manual laborers, climbers, racquet sport athletes, weightlifters, plumbers, carpenters, and even desk workers who perform repetitive gripping. The common thread is repetitive forearm flexor loading, not the sport itself.
How long does a clinical assessment for golfer’s elbow take?
A thorough clinical assessment — including history, AROM/PROM testing, manual resistance, and palpation — can be completed in 10–15 minutes as part of a broader musculoskeletal intake. When differential diagnosis is complex or nerve involvement is suspected, allow additional time and consider referral for imaging or nerve conduction study.
Conclusion: Build a Repeatable Assessment Framework
Assessing golfer’s elbow is straightforward when you apply a systematic, layered approach: start with active range of motion to identify pain-producing movements, follow with passive motion to isolate the tensile component, use manual resistance to confirm tendon involvement, and anchor everything with focused palpation at the medial epicondyle.
The key clinical principles to remember:
- AROM and PROM of wrist/finger flexion and extension are your first screening tools
- Resisted wrist flexion is your most specific manual test
- Palpation localizes the lesion
- Differential diagnosis — always screen for distal tendinitis, cubital tunnel syndrome, and MCL involvement
- Imaging is confirmatory, not primary, in most cases
When you identify golfer’s elbow early and accurately, you set the stage for more effective treatment — whether that’s manual therapy, therapeutic exercise, or a referral pathway for more complex cases.
👉 Related Reading:
- What Causes Golfer’s Elbow? The Anatomy of Overuse Explained — Internal link suggestion
- What are the signs and symptoms of Golfer’s Elbow? — Internal link suggestion
- How to Treat Golfer’s Elbow with Manual Therapy — Internal link suggestion
- What are the self-care and medical approaches to Golfer’s Elbow? – Internal link suggestion
About the Author
This article was developed by the clinical education team at LearnMuscles, founded by Dr. Joseph E. Muscolino, DC — a chiropractic physician, educator, and author with over 30 years of experience in musculoskeletal anatomy, kinesiology, and manual therapy. Dr. Muscolino is the author of multiple widely used textbooks including Kinesiology: The Skeletal System and Muscle Function and The Muscle and Bone Palpation Manual, and has taught continuing education for massage therapists, physical therapists, and chiropractors internationally. The LearnMuscles continuing education platform hosts over 4,000 video lessons for licensed practitioners.
Sources and References
- Gabel, G. T., & Morrey, B. F. (1995). Operative treatment of medial epicondylitis: Influence of concomitant ulnar neuropathy at the elbow. Journal of Bone and Joint Surgery, 77(7), 1065–1069.
- Ciccotti, M. C., Schwartz, M. A., & Ciccotti, M. G. (2004). Diagnosis and treatment of medial epicondylitis of the elbow. Clinics in Sports Medicine, 23(4), 693–705.
- Shiri, R., & Viikari-Juntura, E. (2011). Lateral and medial epicondylitis: role of occupational factors. Best Practice & Research Clinical Rheumatology, 25(1), 43–57.
- Walz, D. M., Newman, J. S., Konin, G. P., & Ross, G. (2010). Epicondylitis: pathogenesis, imaging, and treatment. RadioGraphics, 30(1), 167–184.
- de Smedt, T., de Jong, A., Van Leemput, W., Lieven, D., & Van Glabbeek, F. (2007). Lateral epicondylitis in tennis: update on aetiology, biomechanics and treatment. British Journal of Sports Medicine, 41(11), 816–819.
- Ahmad, Z., Siddiqui, N., Malik, S. S., Abdus-Samee, M., Tytherleigh-Strong, G., & Rushton, N. (2013). Lateral epicondylitis: a review of pathology and management. The Bone & Joint Journal, 95-B(9), 1158–1164.
