
Two groups of specialists who will almost certainly never share a lunch table gave us, without knowing it, the same warning. The way a seasoned manual therapist teaches you to read a body turns out to rhyme, almost word for word, with the way computer scientists are learning to trust a machine.
We set out to do something that sounds like a party trick: put the assessment advice of master anatomy and manual-therapy educators next to the reliability advice coming out of the artificial-intelligence research world, and see whether the two had anything in common. We assumed the answer would be “not much.” One camp talks about fascia, palpation, and the sacroiliac joint. The other talks about parameters, benchmarks, and token probabilities.
Instead, one pattern surfaced so cleanly that it changed how we think about both fields: accuracy is a property of agreement and context—not of any single authority, no matter how good that authority looks on its own. Here is how the two groups arrived at the same place from opposite ends of the room.

What the anatomy experts actually teach
Ask any experienced instructor how confident you should be in a single palpation finding, and you will not get a confident answer back. You will get a caution. The best educators in manual therapy hammer one lesson above almost all others: a lone test, felt once, on one landmark, is not a diagnosis. It is a data point—and a noisy one.
The literature backs the caution hard. A systematic review of manual palpation reliability in patients with low back pain found that agreement between clinicians on soft-tissue and bony-landmark palpation was, in the authors’ words, poor to inconsistent—with reliability scores frequently falling below the threshold that counts as even weak agreement. The reviewers were blunt about the takeaway: because so little is known about the standalone validity of these tests, their clinical usefulness in isolation is uncertain.
That does not mean palpation is worthless. It means palpation is a vote, not a verdict. This is exactly why skilled clinicians triangulate: they combine patient history, active and passive range of motion, orthopedic tests, and palpation, and they look for the story those inputs tell together. When four independent readings point the same direction, you have something. When one shouts and the others shrug, you keep looking. The expertise is not in trusting the hand—it is in knowing that the hand is one witness among several.
The master clinician’s real skill isn’t a magic finger. It’s the discipline of never letting a single signal speak for the whole body.
What the AI researchers found—by accident, at first
Now cross the room. Over the last two years, one of the most stubborn problems in artificial intelligence has been that language models state wrong things with total confidence. In OpenAI’s 2025 analysis of why language models hallucinate, researchers showed that on a factual-recall test, a model that almost never said “I don’t know” produced a wrong answer roughly three-quarters of the time it spoke—while barely losing any accuracy compared with a more cautious model. The confident one wasn’t more correct. It was just more willing to guess.
The reason is structural. A 2026 paper in Nature arguing that grading models only on accuracy actively rewards confident guessing made the point that our own evaluation habits train machines to bluff—the same way a student bubbles in a random answer rather than leave a question blank. A single model, in other words, has a built-in incentive to sound sure even when it isn’t. That should feel familiar to anyone who has watched a nervous student palpate a landmark and announce a finding they don’t actually feel.
So what fixed it? Not a bigger, smarter, lonelier model. The fix was consensus. When researchers stopped relying on one model and instead polled several, then kept the answer the majority agreed on, reliability jumped. In a 2025 study on using model ensembles for content categorization, a single best-performing model scored 0.55 on the accuracy measure. Pool ten models and take the majority answer, and the score climbed to 0.92—a gain of roughly two-thirds. Even a modest panel of two or three models delivered a meaningful jump on its own.
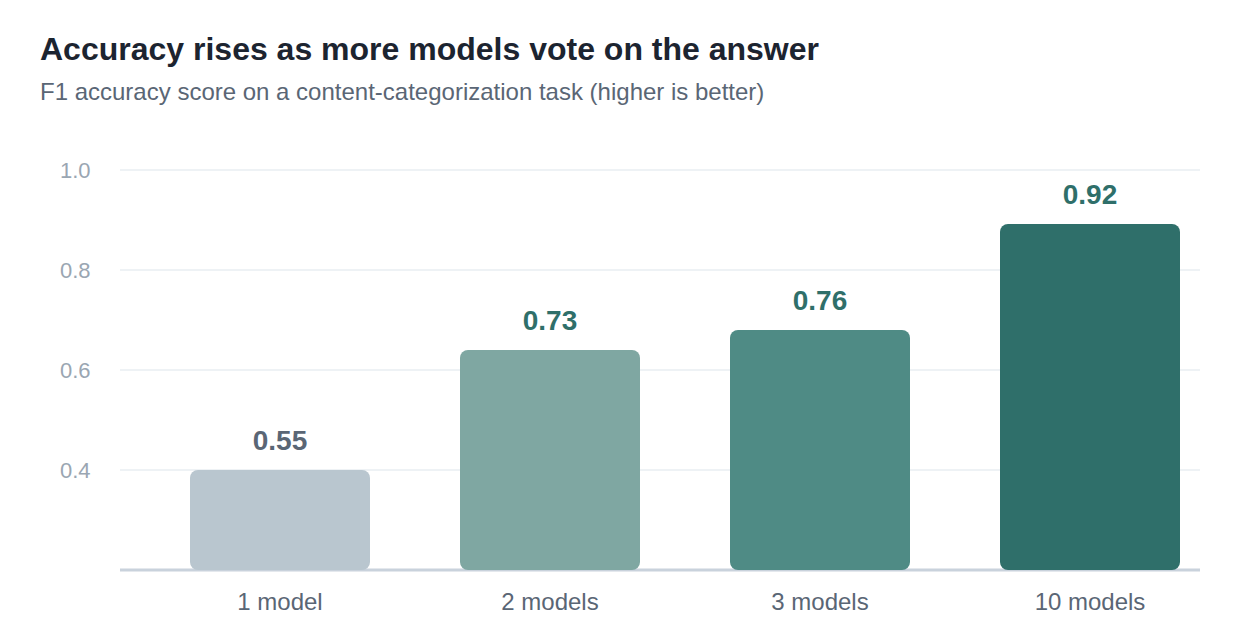
The single strongest model was wrong far more often than a panel that voted. Data: 2025 LLM-ensemble categorization study (see sources).
Read that back with a clinician’s ear. One instrument, used alone, is unreliable and overconfident. Several independent instruments, cross-checked and reconciled, are trustworthy. The AI researchers had rediscovered triangulation.
The pattern that stood out
Here is the sentence both camps would sign, even though one wrote it in a treatment room and the other wrote it in a lab:
Trust the agreement, not the individual. And never read a signal without its context.
That second half matters as much as the first. A palpation finding means nothing without the patient’s history and presentation around it; the same tender spot means one thing in a marathon runner and another in a desk worker. AI research landed on the identical caveat—an answer is only as good as the context the system was actually given to reason over. Strip away the surrounding information and even a panel of models will confidently agree on the wrong thing, exactly as a room full of clinicians will if they’re all handed the same incomplete chart.
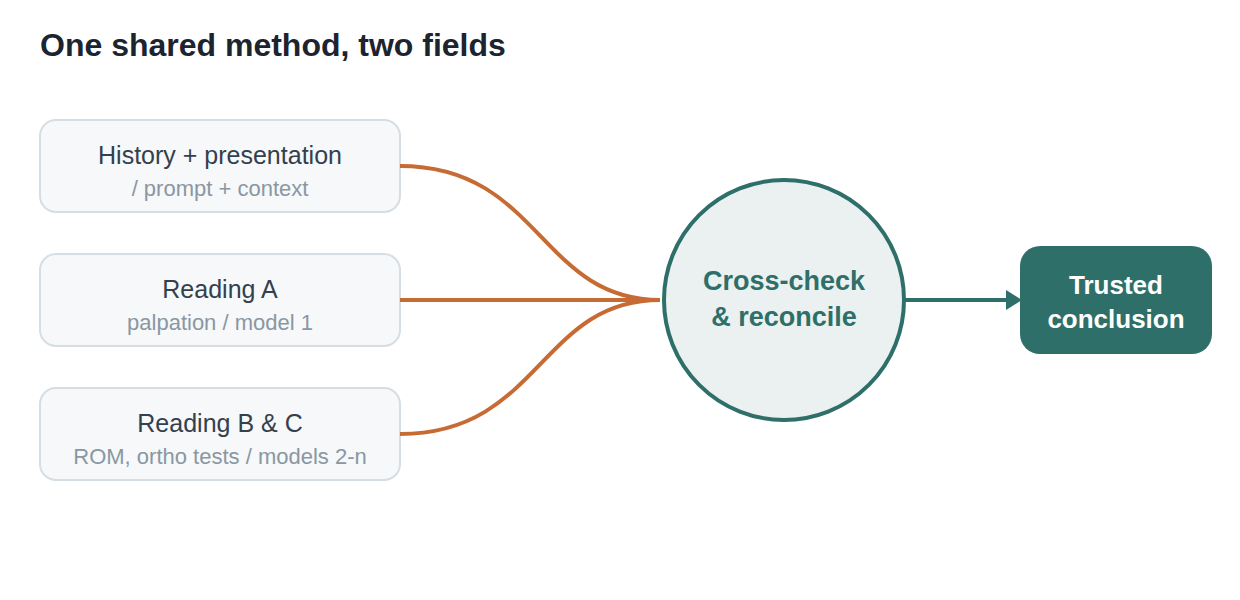
The manual therapist’s workflow and the modern AI-reliability workflow are, structurally, the same picture.
| ~75%
Wrong-answer rate for a confident single model that rarely says “I don’t know” |
+67%
Accuracy gain when a panel of models votes instead of one deciding alone |
<0.6
Typical agreement score for single palpation tests—below the bar for even weak reliability |
Why this belongs in your practice, not just a research paper
The overlap is a nice curiosity, but it earns its keep the moment AI shows up in your actual workday—and for many manual therapists, it already has. You might use a model to summarize a research abstract, draft client-education handouts, rework the wording on an intake form, or explain a home-care routine to a patient who doesn’t share your first language.
That last one deserves real attention. As practices serve more multilingual clients and more educators teach international students, a lot of clinicians now lean on AI to translate intake forms, consent language, and technique instructions. The temptation is to paste text into one engine, copy the output, and move on. But everything above says that’s the palpation-once mistake in a new outfit: you’re trusting a single confident source on material where a mistranslated instruction—”apply pressure” versus “avoid pressure”—has real consequences. Applying the same cross-checking discipline you’d bring to an assessment is exactly what separates a usable translation from a liability, and it’s worth understanding the practical approach to using AI to translate professional material accurately before you rely on it with a client in front of you.
The principle transfers cleanly. Don’t trust one output on anything that matters. Give the system full context, not a stripped fragment. Look for agreement across sources, and treat a lone confident answer the way you’d treat a lone positive test—interesting, unconfirmed, and in need of a second opinion.
A short field guide, borrowed from both camps
Before you trust any single reading—clinical or computational
- Never let one signal decide. A single palpation finding, or a single AI answer, is a vote. Collect a few independent ones before you act.
- Distrust confidence that arrives too fast. The most confident source is often just the one most willing to guess. Certainty is not the same as accuracy.
- Context is part of the reading. A finding without history, or an answer without background, is missing the very thing that makes it meaningful.
- Reconcile, then commit. When your independent sources agree, you have something worth acting on. When they don’t, that disagreement is information—keep looking.
We went in expecting anatomy and artificial intelligence to have nothing to say to each other. What we found instead was a single, portable habit of mind: the people who are best at reading bodies and the people trying hardest to make machines reliable both quietly gave up on the idea of a single infallible source a long time ago. They trust the crowd, in context, cross-checked. It’s a good rule for a treatment room. It turns out to be a good rule for everything else you’ll ask a machine to help you do.
Written by Ashley Cadag
