Myofascial Continuity
 The myofascial continuity (also known as myofascial meridian or myofascial chain) concept suggests that muscles activate along kinematic chains that share common fascial coverings. Anatomic studies have confirmed the existence of these myofascial continuities, in particular the Superficial Back Line Myofascial Continuity. However, there has been little or no research that looks at the function of myofascial continuities in people who are experiencing low back pain (LBP).
The myofascial continuity (also known as myofascial meridian or myofascial chain) concept suggests that muscles activate along kinematic chains that share common fascial coverings. Anatomic studies have confirmed the existence of these myofascial continuities, in particular the Superficial Back Line Myofascial Continuity. However, there has been little or no research that looks at the function of myofascial continuities in people who are experiencing low back pain (LBP).
Comment by Joseph Muscolino
The Superficial Back Line Myofascial Meridian is usually described as comprising the following structural connections from the foot to the head:
- Plantar fascia
- Achilles tendon
- Gastrocnemius
- Hamstrings
- Sacrotuberous ligament
- Thoracolumbar (Thoracodorsal) fascia
- Paraspinal (Erector Spinae) musculature
- Trapezius
- Occipitalis
- Galea aponeurotica
- Frontalis muscle
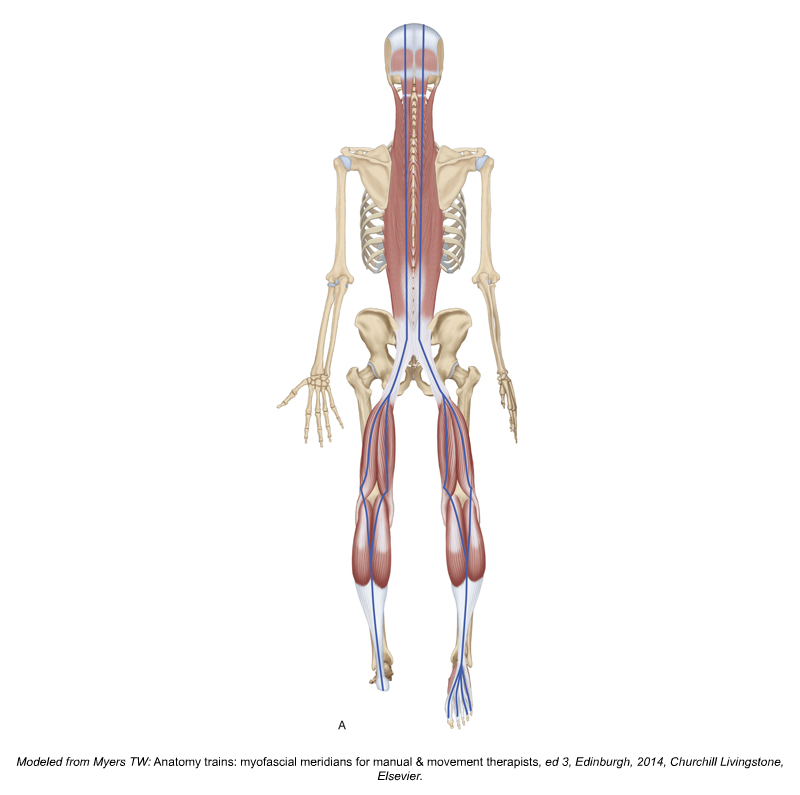
Superficial Back Line Continuity (Myofascial Meridian). Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function. 3rd edition (Elsevier, 2017). Modeled from Tom Myers, Anatomy Trains.
Study of Superficial Back Line Myofascial Continuity and Low Back Pain
Researchers from Haifa, Israel examined muscle activations along the superficial back line in LBP patients compared to healthy controls. The study was published in Journal of Back and Musculoskeletal Rehabilitation.
The study recruited 20 males with chronic LBP, mean age 28.7 ± 3.05 years, and mean BMI 24.91 ± 2.76, along with 17 healthy male controls, mean age 31.06 ± 7.76 years, and mean BMI 23.46 ± 3.43. Muscle activation (gastrocnemius, hamstrings, erector spine, and upper trapezius) along the Superficial Back Line was measured using surface EMG. All subjects underwent five test conditions:
- Condition 1: Passive movement of the right gastrocnemius
- Condition 2: Active movement of the right gastrocnemius
- Condition 3: Active movement of the right gastrocnemius against isometric resistance
- Condition 4: Neck extension without isometric resistance (prone position)
- Condition 5: Neck extension with isometric resistance (prone position)
The main outcome measured was relative muscle activation amplitude between research and control subjects.
Results
The results of the experiment showed muscle activation along the Superficial Back Line that was observed during distant movement (plantarflexion distally or neck extension superiorly). More specifically, during active plantarflexion and during active neck extension, significantly greater muscle activation was found in the low back erector spine musculature of the LBP group than the control group. Muscle activation in other regions of the Superficial Back Line (gastrocnemius, hamstrings, and erector spine at the level of T6) was also observed to be greater in the LBP group than the healthy controls, however the difference was not statistically significant.
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s video streaming subscription service for manual and movement therapists, has six separate folders with video lessons on Manual Therapy Treatment? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
Conclusion
The authors concluded that LBP may cause or result in activation of the low back musculature when contractions occur elsewhere along the Superficial Back Line. The implication of this study is that perhaps therapists should expand the scope of their treatment with patients/clients to include work along the entirely of the myofascial continuity within which pain is present.
Comment by Joseph Muscolino
The concept of myofascial continuities, also known as myofascial meridians (or anatomy trains), has been widely popularized by the work of Tom Myers, including the publication of his seminal book Anatomy Trains. Much of the focus of the myofascial continuity concept has been to look at how lines of tension are transmitted throughout the body. The attention has been primarily focused on how tautness/tightness anywhere along the myofascial continuity may result in that tautness/tightness being transmitted throughout the common fascial sheath, creating a pulling force, in other words tension, throughout the line. This can then result in a loss of flexibility and range of motion more distantly in the body. Therefore, in the world of manual and movement therapy, the attention of myofascial continuity theory has been primarily on the passive tension of the fascial continuity along the line.
However, the present study described here looks at the kinematic chain of myofascial continuities a bit differently. Instead of focusing on the distribution of passive fascial tension forces throughout the line, this study looks at how the presence of pain somewhere along the myofascial continuity line can result in increased facilitation of active muscle contraction (in other words, muscle tightness) elsewhere along the line. This study only looked at this concept applied to the Superficial Back Line in patients with low back pain. However, it does seem to be a reasonable extrapolation that this concept of increased muscle facilitation may occur within other myofascial continuities. Therefore, unless further research is found to disprove this, it seems to be a reasonable conclusion that therapists might be wise to expand their manual and movement therapy to the entirely of the myofascial continuity. Certainly, at the least, the entirely of the line should be assessed to determine if the need for this expanded treatment is valid.
This blog post article was created in collaboration with www.terrarosa.com.au.
(Click here for the blog post article: How Can Tight Hip Flexors Give you a Headache?)
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s video streaming subscription service for manual and movement therapists, has six separate folders with video lessons on Manual Therapy Treatment? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
