Assessment/Diagnosis of golfer’s elbow:
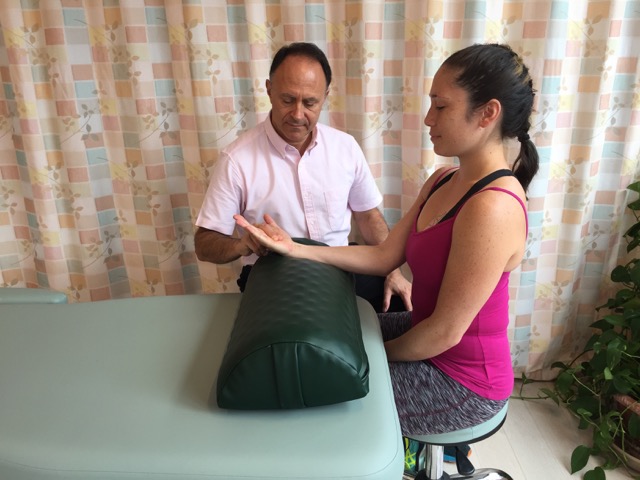
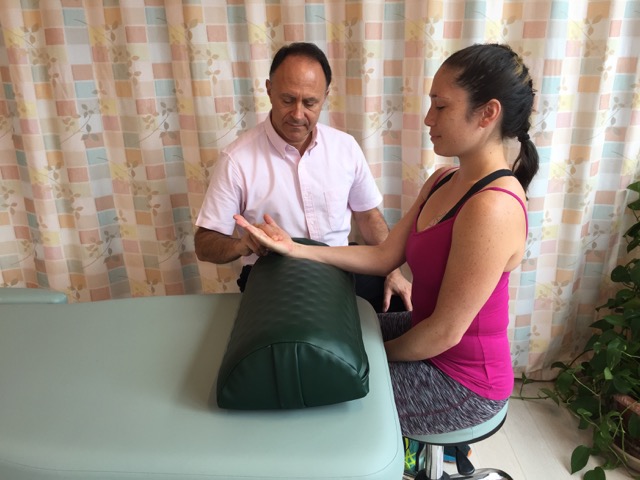
Manual resistance to flexion of the hand at the wrist joint will cause pain (show positive) for a client/patient with golfer’s elbow. Permission: Joseph E. Muscolino.
As stated, knowing how to assess/ diagnose golfer’s elbow (medial epicondylitis / medial epicondylosis) is similar to assessment of tennis elbow and is an extension of our understanding of the underlying pathomechanics of the condition. Active flexion range of motion of the hand at the wrist joint or the fingers at the metacarpophalangeal and proximal interphalangeal joints will likely cause pain because the associated musculature contracts and pulls on the common flexor tendon and the medial epicondyle of the humerus. Active or passive extension of the wrist or fingers would also likely elicit pain because it stretches the associated musculature and therefore pulls on the common flexor tendon and the medial epicondyle. Ulnar or radial deviation might also be painful. Active ulnar deviation would require concentric contraction of ulnar deviators and stretching of radial deviators (passive ulnar deviation would also cause a stretch to radial deviators); therefore either or both muscle groups might show pain. Similar reasoning applies to radial deviation range of motion. Given the irritation, swelling, and degeneration of the common flexor tendon, and the irritation and swelling of the medial epicondyle, palpation would also likely elicit local pain. Swelling at the medial epicondyle might also be visualized; look for the bony contours of the medial elbow to be less evident compared to the other upper extremity of the patient’s/client’s body.
Assessment (diagnosis) of golfer’s elbow is done with active and passive range of motion, manual resistance, and palpation.
Medically, golfer’s elbow is usually diagnosed via ultrasound or MRI. These are the most accurate ways to assess/diagnose the extent of possible degeneration and/or tearing of the common flexor tendon.
Differential diagnosis/assessment of golfer’s elbow:
Golfer’s elbow is a simple and straightforward condition to assess. As with tennis elbow, it is possible for myofascial trigger points (TrPs) to be present without the assessment of golfer’s elbow. However, TrPs are also commonly part of the development of golfer’s elbow as a condition. If tendinitis of wrist and finger flexors is present at their distal tendons at the wrist joint, active and passive ranges of motion will likely show the same positive and negative results as golfer’s elbow during physical examination, however the patient’s/client’s pain will be located distally at the wrist instead of proximally in the forearm near the medial epicondyle of the humerus.
Click here for an article on how to assess (diagnose) tennis elbow.
Note: This is the third of five blog post articles on golfer’s elbow.
The five articles are:
- What are the causes of Golfer’s Elbow?
- What are the signs and symptoms of Golfer’s Elbow?
- How do we assess (diagnose) Golfer’s Elbow?
- How do we treat Golfer’s Elbow with manual therapy?
- What are the self-care and medical approaches to Golfer’s Elbow?
