This blog article is a summation of a one hour and six minute long lecture on pain neuroscience by Dr. Tasha Stanton, a physiotherapist (physical therapist) out of Australia. This is a fascinating lecture that is well worth the time spent to watch it. However, until you find that time, here is a (fairly lengthy and thorough) summation of the lecture, along with a few conclusions and applications added by me.
Pain is in our brain
![]()
The essence of her lecture is that when it come to the experience of pain, what is happening in your brain might be more important than what is happening out in your body (low back, knee, or any other structural part of your body).
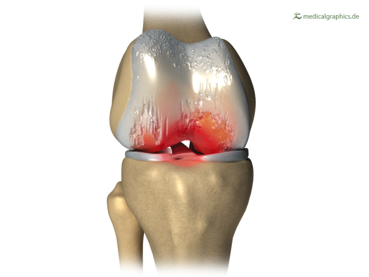
Osteoarthritis (Degenerative Joint Disease) of the right knee joint
She begins by discussing a study in which the amount of knee joint osteoarthritis (OA) does not correlate with the degree of pain experienced in the knee. She shows two knee x-rays, one with a great amount of OA and the other without almost any OA, yet both people presented with a pain level of 5 (on a scale of 0-10). Her conclusion is that what the brain perceives is more important than the actual structural joint damage…
Note: More on this later in the blog, but for right now, I would like to point out that nowhere in her discussion of this study is soft tissue dysfunction mentioned. Might some of the subjective pain experienced by the patients be related to soft tissue dysfunction instead of bony tissue damage, which is all that an x-ray shows?
She uses this study to posit the hypothesis that the degree of pain a person experiences is actually in our brain and not in our knee.
Note: Certainly this is fundamentally true. Pain can only be experienced in our brain, as all sensory perception is experienced in the brain.
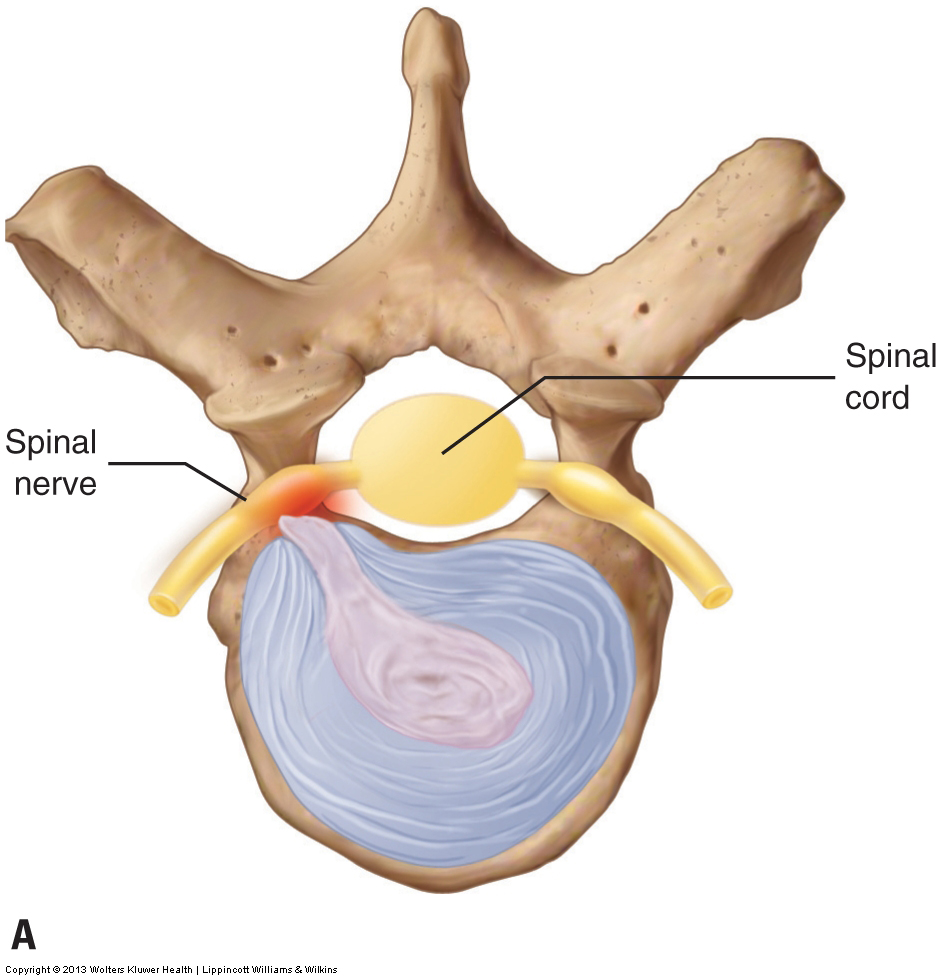
Herniated disc compressing the spinal nerve. Permission Joseph E. Muscolino – Manual Therapy for the Low Back and Pelvis: A Clinical Orthopedic Approach
She then states that 60% of us without low back pain would, if examined with MRI, show low back disc damage. Again, her conclusion is that the degree of pain we experience is more dependent on what the brain perceives than the actual amount of tissue damage in the joint/structure where the pain is perceived to exist.
Note: I agree with this theory. I have long said that there is a “lag” between objective structural damage and subjective symptomology, including pain. If we always experienced every bit of structural damage that we have, we would be in pain all the time. There needs to be some sort of lag, or put another way, threshold above which we must be to experience pain. But I feel that there are limits to all theories/models to explain the functioning and the dysfunctioning of the human body. I feel that pain neuroscience advocates need to be careful to not swing the pendulum so far in the other direction that mechanics in the tissue are totally ignored.
Our brain produces our sensations according to the credible believable evidence…
Tasha Stanton likes to use the following quote to explain her philosophy of pain neuroscience:
“Our brain produces our sensations according to the credible believable evidence that is present, not just according to the sensory information from that body part.”
She follows with the following examples:
Example #1:
A man is brought into the emergency room with a nail skewered into his boot. He is in excruciating pain every time his foot is touched. But when the boot is removed, it is found that the nail had never entered his body, but rather had gone between two toes.
Conclusion: Based on the believable credible evidence, the person experienced pain so that he would not move his foot and possibly cause more damage. In essence, the brain creates pain in response to real or perceived danger as a construct to protect us from doing anything that might further the real or perceived damage.
Example #2:
A study at Oxford showed that the amount of opioid drug that was given to participants who had a burn injury did not perfectly relate to the amount of pain that they experienced. The opioid did decrease pain by 15%, even when they did not know that they were receiving it. But when the people were told that they would be given the opioid, their pain decreased even more. Then when the people were told that they were no longer receiving opioid, but in fact still were receiving it, their pain fully returned. The belief that the opioid was not being given entirely obliterated the effect of the opioid. The results were determined not just by the statements made by the patients but also by imaging the brain of the patients, showing brain activity that correlated with the perceived degree of pain.
Conclusion: The expectancy of pain by the brain is a powerful factor in experiencing pain. Therefore, chronic pain patients/clients who have never experienced relief may enter treatment with the expectancy of not being helped; and this expectancy may then negate any actual help that the therapist provides. The application here is that therapists need to be aware of how they manage their patients’/clients’ expectations.
Example #3:
Another study discussed involved patients with the condition CRPS (Complex Regional Pain Syndrome). CRPS usually follows injury, usually a broken bone, in the affected limb and results in hyperesthesia (increased pain sensitivity) in that limb. As a result, simply being touched in the affected areas of the injured limb would result in pain. The study showed that the patients’ experience of pain was largely correlated to not just being touched but also when they “believed” that they were being touched. This process was done with a “virtual limb” by placing a mirror next to the good limb/hand, which reflected what looked like the injured limb/hand. When they touched the sensitive regions of the injured hand in the good hand, the person experienced paresthesia in the injured hand, even though they intellectually knew it was the good hand that was being touched. Further, when healthy areas of the injured limb/hand were touched on the good hand, the person did not experience any paresthesia in the injured hand.
Conclusion: The apparent perception of danger to the injured limb/hand caused the brain to experience pain in that hand. Given that the patients knew intellectually that the injured hand was not being touched, this process of pain construction in the brain must work at deeper levels in the subconscious brain than intellectual consciousness.
Example #4:
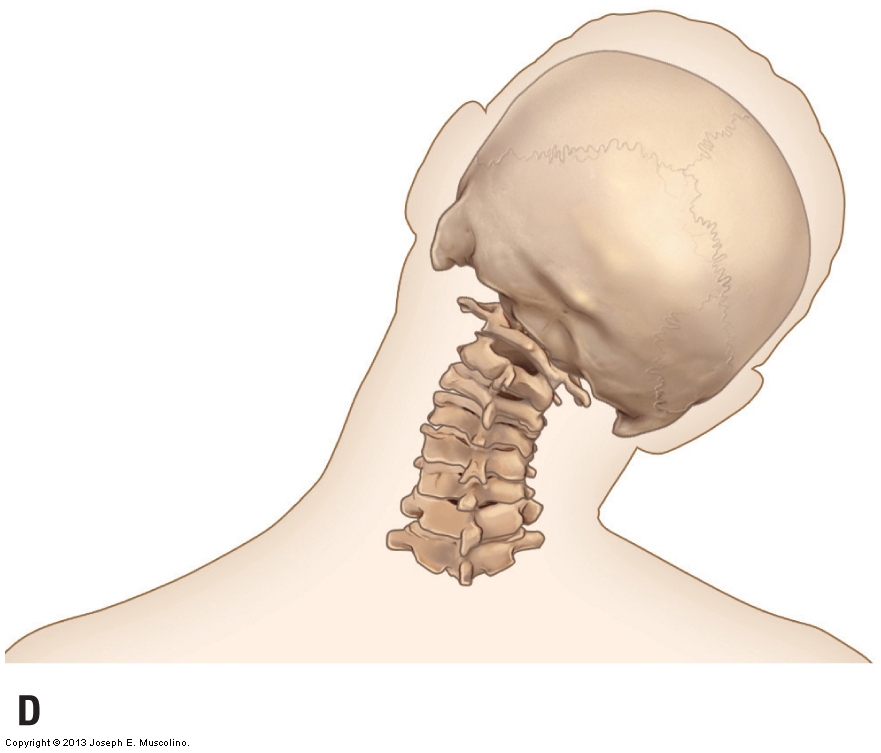
Right lateral flexion of the cervical spine. Permission Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck
Another example involved a study related to people who have mechanical pain in their neck at a certain range of motion (ROM). In other words, at a certain degree of cervical rotation, these people consistently experienced pain in their neck. They were then given video goggles so that the eyes would “lie” to the person by altering the landscape that they would see so that they would believe that they had either moved more or less than they actually had. The results were fascinating. When the goggles told them that they had moved more than they actually had, they experienced pain at a lesser ROM because they believed that it had been the greater ROM that they associated with the onset of pain. And when the goggles told them that they had moved less than they actually had, they were able to increase their ROM before experiencing pain.
Conclusion: Mechanical ROM of the neck (and this could likely be extrapolated to any joint) alone is not the only factor involved in experiencing pain. Rather, the belief of ROM is also a strong cue for when the person perceives the pain.
Neurophysiology of Pain
Dr. Stanton then discusses the neurophysiology of pain:
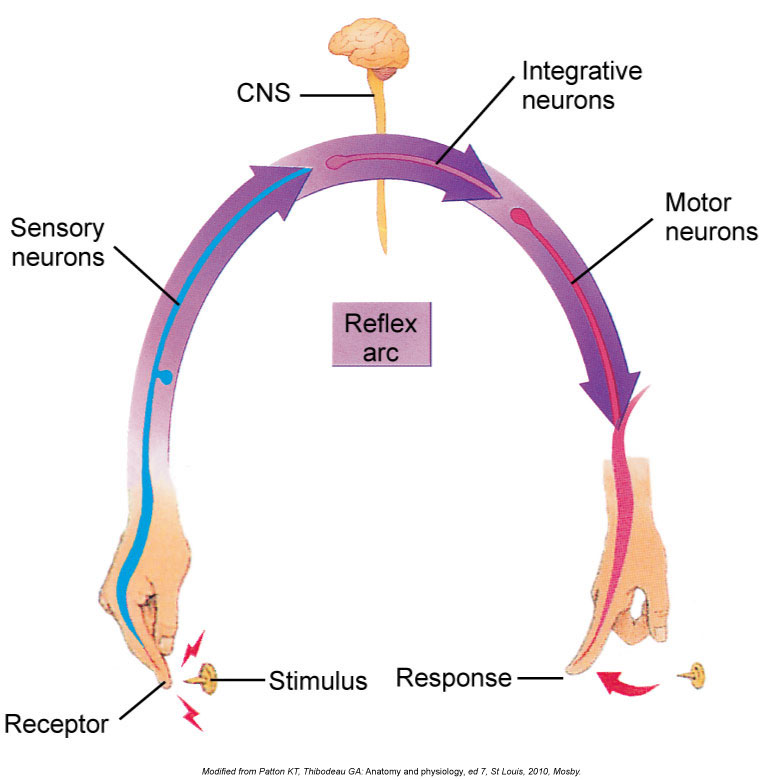
Pain reflex arc. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3ed. (Elsevier)
Classic wisdom is that if you step on a thumb tack, nociceptors (thought of a pain neurons) send a message of pain up to the brain. She posits that the message is not yet a message of pain but rather is a message of danger that the brain then associates with other factors to determine that pain is felt.
Note: I agree that this the association of danger would increase the experience of pain. But I feel that the statement is a little to black and white here. Would a newborn baby with little or no life experience, and therefore has few if no associations of what constitutes danger, not experience pain if a painful/noxious stimulus (such as having a needle pierce its body) occured, especially if, for example, the painful stimulus were out of its line of sight? Although this study could not and should not be done for humane reasons, it would stand to reason that many newborns have probably experienced such noxious stimuli and been noticed to react by crying, which would seem to be good indicator of overt pain, and not just perceived danger (given that being a newborn, they do not have these learned associations of danger).
To be fair, she does then qualify this concept by then discussing how the brain can regulate/modulate the perceived pain in the nociceptors by facilitating or inhibiting them. So the construct is changed from an all or nothing to a shade of gray by modulation.
Chronic Pain Patients/Clients
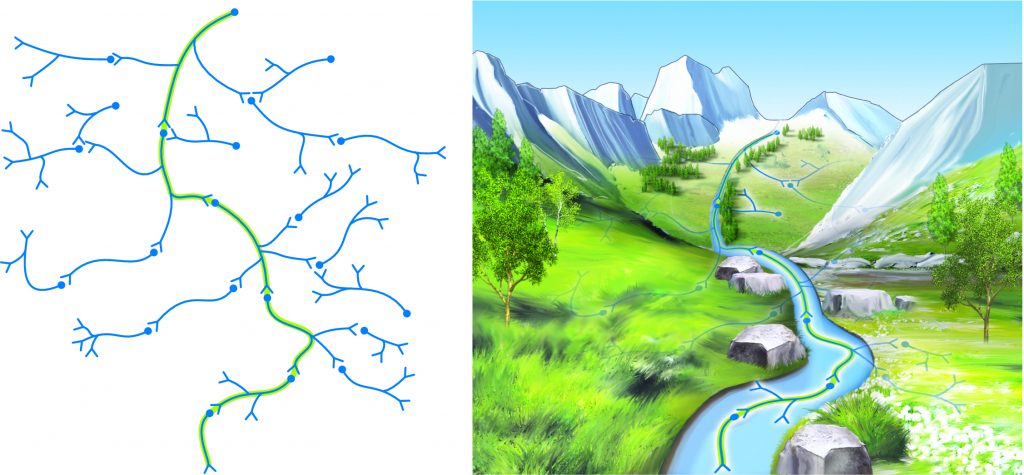
Consolidation of a neural pathway memory pattern is analogous to water etching a deeper and deeper pathway into the side of a mountain over time.
She then draws the distinction between acute pain patients and chronic pain patients. She introduces the idea that the concept of pain neuroscience can be strongly related to the patients with experiencing chronic pain, in whom the association of danger related to pain is has been repetitively entrenched within their nervous system. This concept of amplifying the signal of pain is known as “central sensitization” of pain, which is a mechanism of nervous system neural plasticity that has long been accepted.
She gives a very nice analogy that if you turn up the volume of the radio, the person speaking on the radio has not actually started speaking louder, you have simply increased the amplitude of the sound that you hear. Similarly, central sensitization of pain amplifies the signal of pain so that signals that would not have been experienced as pain now are. In other words, otherwise subthreshold sensory signals now are over the threshold and do actually cause pain. So a lesser stimulus such as a simple touch might actually cause pain in a chronic pain patient. So now the sensory signals no longer correlate to the actual degree of tissue damage that is occurring. In essence, this is a case of the brain becoming hypervigilant in an effort to try to protect the person from possible damaging experiences.
She states a famous quotation regarding nervous system learning:
“Neurons that fire together, wire together.”
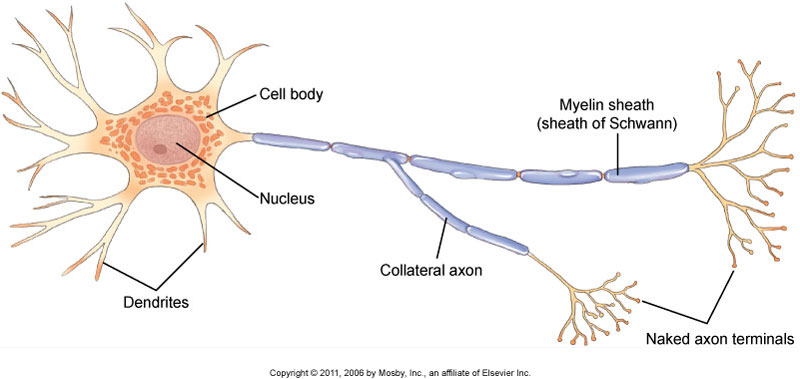
Neuron figure. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3ed. (Elsevier)
She discusses the example of a person who has anxiety because they are afraid that bending will cause low back pain. Because anxiety has now become associated (wired) with low back pain, whenever they have anxiety for any other reason, they will experience low back pain. This explains why so many people has characteristic pain patterns whenever they become stressed. These pain patterns could be low back pain, headaches, tight necks, stomach aches, or any other physical manifestation of anxiety/stress-induced pain.
She brings up an application of this for physicians. If we tell a patient that their MRI shows a herniated low back disc, and especially, then the patient might experience greater pain because of what they now believe to be the danger to their health. The conclusion here is that it is incumbent upon physicians and therapists to not “alarm” the patient when describing the results of physical examination. It should be explained that greater pain does not necessarily relate to the degree of actual tissue damage in the body. She discusses a study that showed that when patients were taught about this concept of pain sensitization that greater pain might not actually represent their tissue damage, these patients then had immediate functional improvement compared to the patients who were not taught about pain sensitization.
Altered Body Image
Dr. Tasha Stanton then discusses how studies have shown how chronic pain patients lose proper proprioceptive input of their position in space and movement through space, their two-point perception of touch, and also the perception of the relative sizes of their healthy versus unhealthy body parts. In other words, they begin to lose the entire perception/image of their body.
Being aware of this alteration in perception can actually be used to help the chronic pain patient by reversing this association. It has been shown that if we can improve the patient’s perception of their body, their pain level decreases. She discusses a number of applications that neural pain science therapists might employ using visual illusions that change the patient’s perception of their body image and movement, which then result in decreased pain. This application of this work is described as “sensory and motor precision training.” In other words, “body-relevant information can modulate pain.”
But we might be able to apply this concept to manual and movement therapies. Manual and movement therapists/instructors/trainers might improve their client’s pain level by improving the client’s perception of touch by manual therapy (e.g., massage therapy) and movement by movement therapists (e.g., Pilates and yoga instructors, fitness trainers).
The Brain Creates Pain to Protect us from Injury / Tissue Damage
Dr. Stanton then expands this concept of pain as being a construct of the brain to protect us from possibly further hurting ourselves to describing a study in which stiffness has also been found to not be totally dependent on the actual objective mechanical function/dysfunction of the tissues of the body. In other words, the brain can also modulate our perception of stiffness, making us believe that we are stiffer than we really are, with the intended goal of limiting out movement so that again, we do not cause possible further damage. She cites a study that related stiffness to pain and found that people with back pain overestimated how much they were actually moving by 60%. In other words, people with chronic back pain “feel” stiffer than they actually are.
OVERALL CONCLUSIONS
I do not believe that there is any doubt that the brain is involved in the perception of pain.
- As she states, “Our brain produces our sensations according to the credible believable evidence that is present, not just according to the sensory information from that body part.”
- That neurons that “fire together wire together,” creating associations of pain with other factors.
- That central pain sensitization does play into the degree of the pain that the chronic pain patient/client experiences.
- That in chronic pain patients/clients, there are measurable changes in their brain functioning.
That therefore, to some degree, pain is a construct of the brain to protect us from possible further damage.
Therefore, when we treat out patients/clients, we need to treat their body AND their mind. I believe that most therapists in the world of alternative health already recognize that there is a mind-body connection. Dr. Tasha Stanton does a beautiful job of describing how science is beginning to understand that the mind-body connection relates to the experience of pain.
So I believe that understanding “pain neuroscience” theory is important to understand and apply. When we treat our patients/clients, we need to be aware that we are treating their body and their mind.
BUT, as with all excellent theories/approaches to treating our patients/clients, it is important to not exaggerate it and follow only this belief at the exclusion of all others. In other words, even though the brain can strongly modulate the experience of pain (and even stiffness), the mechanical factors in the periphery ARE still important. In other words, the role of manual and movement therapists to affect the mechanics of myofascial-skeletal tissues is still extremely important!
(Click here for a blog post article on Neural Plasticity.)
