
This blog post article is part of a series of articles on assessment of the low back and pelvis. Scroll to the end of this article to see the others in this series.
Straight Leg Raise Tests
Following are the straight leg raise (SLR) orthopedic assessment tests that are used to assess pinched nerve conditions caused by a space-occupying lesion.
- Active SLR (ASLR)
- Passive SLR (PSLR)
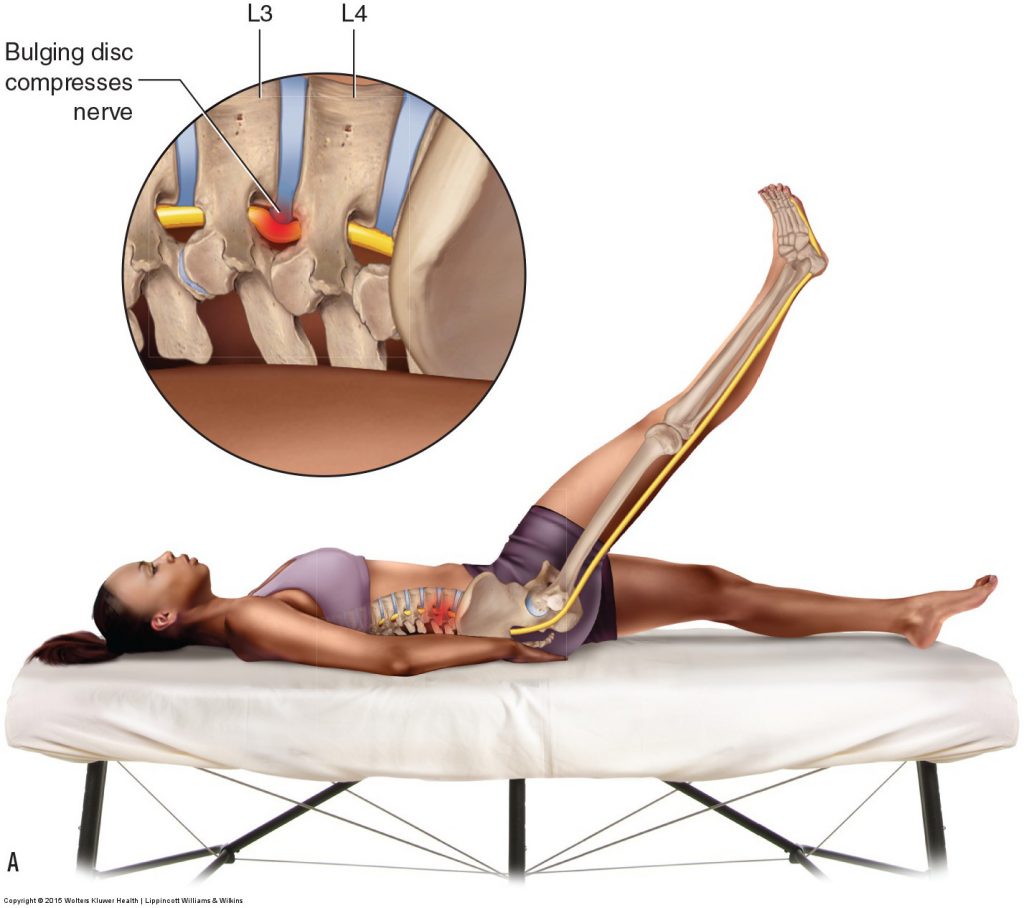


Figure 6. SLR tests. (A) Active SLR. (B) Passive SLR. (C) Full SLR test. SLR tests tense and pull long the sciatic nerve. If a space-occupying lesion is present, such as a bulging disc as seen here, compression of the associated nerve can occur, causing sensory symptoms into the lower extremity on that side. Permission Joseph E. Muscolino DC. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015)
Both active SLR and passive SLR tests are designed to pull long and taut the sciatic nerve on the posterior side of the body. If a space-occupying lesion in the lumbar spine such as a pathologic disc or bone spur is encroaching into the central canal or the intervertebral foramen, a nerve root that contributes to the sciatic nerve will be pulled against the encroachment and compressed (pinched nerve). This compression can refer symptoms into the lower extremity.
Active SLR test is performed by asking the client to actively raise the thigh into flexion at the hip joint while keeping the knee joint fully extended. Passive SLR test is performed in a similar manner except that the client is passive as the therapist moves the client’s lower extremity. In each case, it is important that the knee joint remains fully extended (hence the name straight leg raise) (Fig. 6A). Passive SLR is probably more effective at assessing a space-occupying condition because there are fewer parameters given that muscle contraction is not occurring. If flexion is introduced into the knee joint, tension on the sciatic nerve will be lost, and it will be slackened and no longer compressed against the disc or bone spur. Compression of the sciatic nerve against the space-occupying lesion can cause sensory symptoms such as pain or tingling to refer down into the lower extremity (buttock, thigh, leg, and/or foot). SLR test for a space-occupying condition is considered to be positive if lower extremity referral symptoms are experienced.
- It is important for the client to discern between referral symptoms of a pinched nerve (in effect, sciatica) from the sensation of tight hamstring musculature.
- It is also important to note that local low back pain alone does not constitute a positive SLR test for a space-occupying lesion (local pain can occur with SLR if the client has a sacroiliac or lumbar sprain or strain, or sacroiliitis); lower extremity referral symptoms must occur for a space-occupying lesion to be assessed.
- And it should be pointed out that compression of the sciatic nerve due to a tight piriformis (piriformis syndrome) may also yield a positive with SLR.
- SLR test to assess a space-occupying condition can be performed actively or passively because the same mechanism of pulling long the sciatic nerve occurs in either case; however, as mentioned above, it is probably more discerning to perform SLR passively, so passive SLR is most often performed when assessing for a pinched nerve from a space-occupying lesion.
Note: Straight Leg Raise
Straight Leg Raise (SLR) assessment requires the client to be able to flex the thigh at the hip joint while maintaining the knee joint in full extension. This posture is extremely difficult for a client who has very tight hamstrings because hip joint flexion and knee joint extension stretch these muscles. If the client’s hamstrings are so tight that the client cannot bring the thigh very far up into flexion, then the SLR test is not valid because sufficient tension could not be placed on the sciatic nerve to assess a space-occupying lesion. It is also important to make sure the client does not compensate for tight hamstrings by posteriorly tilting the pelvis; doing so would diminish the tension on the sciatic nerve, thereby lessening the efficacy of the SLR assessment test.
SLR test can be augmented to become full SLR test by adding in adduction of the thigh at the hip joint, dorsiflexion of the foot at the ankle joint, and eversion of the foot at the subtalar joint (Fig. 6B). The idea behind full SLR test is that these added joint postures increase the tension on the sciatic nerve. Thigh adduction stretches the entire sciatic nerve around the ischial tuberosity as it crosses the hip joint. Dorsiflexion and eversion of the foot increase the stretch tension on the tibial nerve portion of the sciatic nerve because the tibial nerve enters the foot by crossing the ankle joint region posteriorly and medially.
(Click here for a blog post article on orthopedic assessment of space-occupying lesions of the neck.)
This blog post article is the ninth in a series of 18 blog posts on the subject of assessment of the low back and pelvis.
The blog post articles in this series are:
- Introduction to Assessment of the Low Back and Pelvis
- Health History
- Introduction to Physical Assessment Examination of the Low Back and Pelvis
- Postural Assessment of the Low Back and Pelvis
- Range of Motion and Manual Resistance Assessment of the Low Back and Pelvis
- Muscle and Bone Palpation of the Low Back and Pelvis
- Joint Motion Palpation Assessment
- Overview of Special Orthopedic Assessment Tests of the Low Back and Pelvis
- Straight Leg Raise Tests for Space-Occupying Lesions
- Cough Test and Valsalva Maneuver
- Slump Test
- Piriformis Stretch Test
- Straight Leg Raise and Manual Resistance Tests for Strains and Sprains
- Nachlas and Yeoman’s Tests
- Sacroiliac Joint Medley of Tests
- Treatment Strategy for the Low Back and Pelvis
- Self-Care Advice for the Client with a Low Back / Sacro-Iliac Joint Condition
- Brief Review of Assessment and Treatment of Conditions of the Low Back and Pelvis
