
Introduction
A recent article published in Journal of Bodywork and Movement Therapies by authors from Israel attempted to objectively define deep tissue massage to provide an evidence-based therapy. However, massage therapist and instructor, Art Riggs, commented that gallant as their effort is, the task of defining deep tissue massage is not only impossible, but is unproductive.
Deep tissue massage (DTM), is a term commonly used as a form of “deep” therapeutic massage, but the term was also used loosely implying many different modalities. It is unclear what elements define DTM and makes it unique. Researchers from Department of Physical Therapy in Ben-Gurion University of the Negev, in Israel attempted to clarify this by conducting an evidence-based research on DTM to establish its efficacy and safety.
The Definition of Deep Tissue Massage
Not surprisingly, the researchers cannot find a commonly accepted definition of deep tissue massage in the literature.
Steve Capellini and Michel van Welden in their book “Massage for Dummies” jokingly gave a non-massage definition of Deep Tissue as Kleenex stuck deep between the cushions on your couch.
In massage therapy, some referred DTM as “myofascial release” (MFR), “trigger point therapy” and “neuromuscular therapy” while others consider it as the application of Swedish massage strokes using strong pressure.
Carole Osborne-Sheets in her book Deep Tissue Sculpting states: “ …. as a generic category, myofascial work includes sculpting, structural imbalance, self-massage … it also includes Rolfing, Chua k’a, Lomi-Lomi, Hellerwork, postural integration, MFR, trigger point therapy …”.
The authors suggested the term DTM is commonly used to describe the intention or aim of the therapist to target a deep tissue by applying a greater pressure or force. To avoid confusion, the authors suggest differentiating the terms “deep massage” and “deep tissue massage”.
Joseph E. Muscolino, CE Educator. Clinical Orthopedic Manual Therapy (COMT) Certifications. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015)
Deep massage can also be used to describe the intention of the therapist to treat deep tissue by using any form of massage.
Meanwhile, deep-tissue massage should be used to describe a specific and independent method of massage therapy, utilizing the specific set of principles and techniques as defined by Art Riggs in his book Deep Tissue Massage: “The understanding of the layers of the body, and the ability to work with tissue in these layers to relax, lengthen, and release holding patterns in the most effective and energy efficient way possible within the client’s parameters of comfort”.
The authors particularly endorsed Art Riggs’ definition which has the following principles:
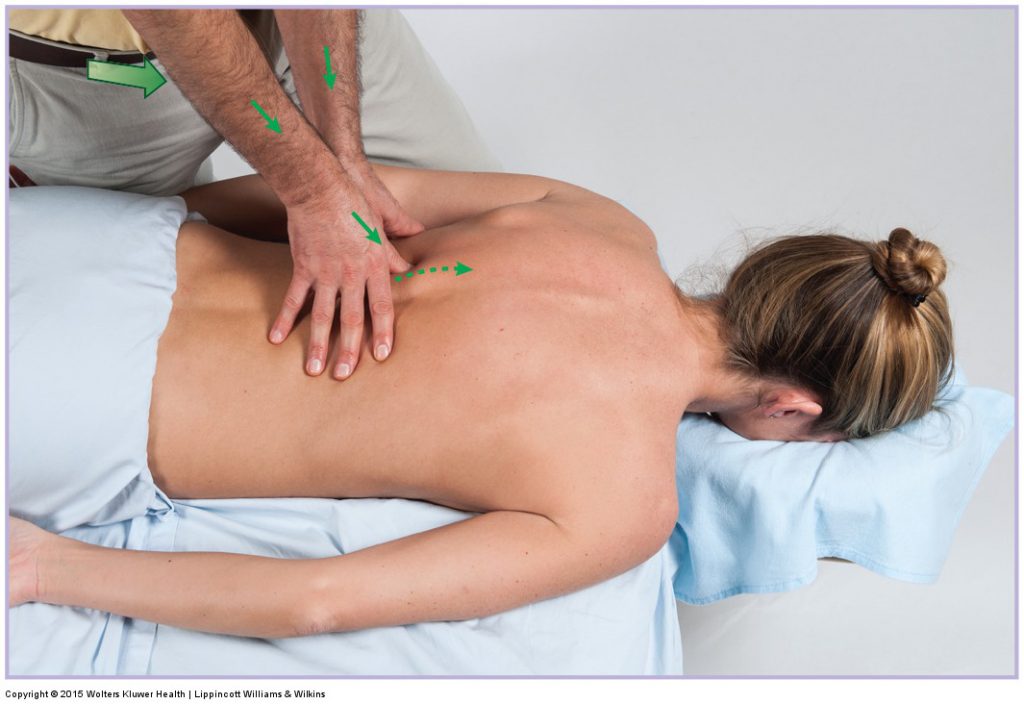
- Slow strokes.
- Diagonal applications (except for treating myofascial trigger points).
- Maintaining depth of treatment according to targeted tissue.
- Understanding of the differences between deep and forceful applications.
- Using body weight to generate the force transmitted through the hands, knuckles or elbows.
- When working on a muscle belly parallel and cross-fiber strokes should be included.
- Include stretching or activation of muscle.
- Special attention to attachments of muscles.
- The application should be within the client’s parameters of comfort (minimally painful or no pain at all).
As for the root techniques, the authors again quoted Art Riggs (2007) “… deep tissue techniques … are based upon broad principles of massage, and must be taught in that context”. For instance, pressure application can be perpendicular, oblique or transverse to muscle fibers, depending on the desired outcome, and still be considered DTM. On the other hand, these principles can be identical to other forms of massage which are not DTM. They stressed that techniques are not method-specific.
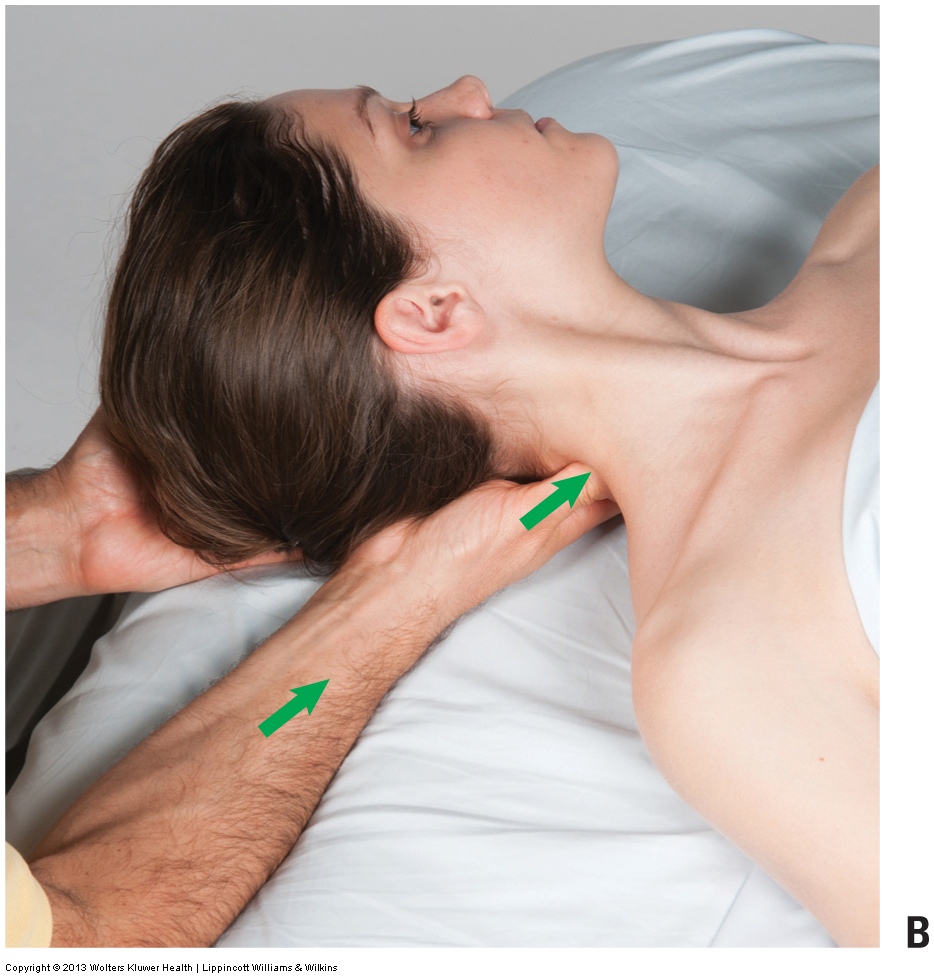
Joseph Muscolino, CE Educator. Clinical Orthopedic Manual Therapy (COMT) Certifications. Permission Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck (2013).
Evidence-based
The authors from Israel tried to find clinical studies on DTM. However, they were confounded by the heterogeneity of techniques and protocols used in published studies. The authors listed some studies on myofascial trigger point treatment, which may be part of DTM, but not necessarily following the principles as stated above.
The authors first evaluated the effect of DTM on heart-rate and blood pressure. Two studies listed in the review seem to be interesting and relevant, Cambron et al. (2006) defined DTM as the intention to access deep layers. In their case series, it was demonstrated that some forms of massage can cause a decrease in blood pressure while others cause an increase. What the authors defined as DTM did not influence blood pressure. In contrast, trigger point therapy caused a minor increase in blood pressure.
Ce et al. (2013) evaluated the efficacy of five modalities in recovery after a heavy-duty cycling exercise by using deep and superficial massage as two of the modalities. Their definition was based on the intention of the therapist. Preliminary measurements showed that therapists apply 650 N/m2 for deep massage and 190 for superficial. The authors found that neither a deep nor superficial massage influenced recovery rate. They also found that stretching and deep and superficial massage do not influence blood lactate levels after heavy-intensity cycle exercise.
The authors found few studies that showed favourable outcomes from deep tissue massage in pain populations (such as chronic low back pain).
In particular, a study by Frey Law et al. (2008) used delayed onset muscle soreness as a model to evaluate the efficacy of DTM for “deep muscle pain.” In this study, the authors demonstrated that both DTM and a superficial massage were able to reduce hyperalgesia (elevated pain pressure threshold), but only DTM reduced stretch pain (with only 11 mm difference between the groups). In this study, the term DTM was used to describe the intention to treat deep tissue with the application of “deep kneading.” A few studies also show various forms of DTM can help patients with decreased range of motion.
Nevertheless, there were are few rare but serious adverse events that were found related to deep tissue massage, mostly as a result of the forceful application of massage therapy.
The authors ended the paper by stating “future research on massage therapy should be based on a common definition, classification system and the use of common comparators as controls.”
Comments by Art Riggs

Author, therapist, and instructor Art Riggs was amused to find his writings referenced in a scientific article, stating, “I’ve forever been confused about what deep tissue massage actually is, both in my therapeutic work and in teaching.”
Two different clients with different issues would probably have very different definitions of the work.
The authors of the article do a fine job of attempting to define an unquantifiable skill. Gallant as their effort is, I feel the task of defining deep tissue massage is not only impossible, but is unproductive. The line along the continuum between “regular” and deep tissue massage is not sharp and can’t be clarified by a list of techniques. I remember great debate 35 years ago about whether to call one’s self a massage therapist or a bodyworker, not only for one’s ego, but as a reason to charge more for doing bodywork.
An accurate description of the practice should not only cover the varied eclectic techniques and philosophies that they list, but also some of the things that exclude work from being classified as deep tissue massage. I do like the authors’ distinction between deep massage; (the all-too-common practice of performing any form of massage while simply pressing harder) and offering a different form of therapeutic bodywork called deep tissue massage based upon advanced training and emphasis upon varied goals and strategies.
In reality, the term deep tissue is actually misleading; many of the techniques that they list actually may be performed in other modalities and often treat superficial tissue.
- Superficial fascia release—Ask any Rolfer® or myofascial specialist working with superficial fascia, and they may strongly deny that they are performing deep tissue massage, although fascial work is usually involved in deep tissue protocol.
- Working on superficial muscles such as pectoralis major; any of the muscles of the rotator cuff; specific muscles of the arm and leg including the iliotibial band; and of course, dozens of other superficial muscles that need skilful work to align, lengthen, and patiently release adhesions rather than just squeezing.
- Conversely, a great amount of the skill of deep tissue massage does, indeed, entail the skill of working through superficial tissue to access deep restrictions. Examples would be isolating pectoralis minor deep to pectoralis major, focusing work on the deep rotators under gluteus maximus, and flexing the knee to shorten and soften gastrocnemius for easy access to soleus.
- Accessing deep tissue does not necessarily imply that the work has to apply a lot of pressure under the “no pain/no gain” fallacy. Work to deeper layers can be quite subtle and is different from hard pressure.

Joseph Muscolino, CE Educator. Clinical Orthopedic Manual Therapy (COMT) Certifications. Permission Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck (2013).
The length of this response prevents giving details of specific techniques, so I will confine myself to discussing the broader issue of “evidence-based research” which by definition is constrained by its attempt to control multiple complex factors of techniques, strategies, variations in patient symptoms, and therapeutic benefits into strict parameters to study results. The whole in deep tissue massage is much more than the sum of the parts.
One could easily add (or subtract) many of the authors’ specific techniques and strokes such as trigger point, cross-fiber friction, stretching, etc. that would fall not only under the umbrella of deep tissue massage, but other modalities. Like the clubs in a golf bag, the actual techniques often have less to do with the specific club one chooses and a lot more to do with the terrain, the actual symptoms being treated, their causes, the indefinable skill of touch, intuition and creativity that the therapist uses to satisfy the needs of the human being behind the symptoms. Attempting to strictly control these factors under the guise of evidence-based research seems futile and misleading.
It seems crucial to distinguish between a limited academic list of techniques and the actual practice of giving a deep tissue massage SESSION in real life, based upon a blending of the therapist’s skill, the wildly varied public perception of proper deep tissue therapy, and the individual needs of the client.
Practical Applications
Let’s leave this topic of definition and semantics of deep tissue massage and discuss some practical applications for a bodywork practice. The tools and philosophy of a deep tissue practice are so varied that each practitioner must be thoughtful about blending their individual expertise (having an eclectic tool box, but not being a “jack of all trades/master of none”) and philosophies to satisfy clients’ varied definitions of a deep tissue massage.
I hear three basic complaints from the public about Massage:
- By the numbers /one size fits all routines or protocols for everyone that don’t address the needs of clients, sometimes called McDonald’s massage.
- Excellent general massage that feels good at the time but does not address the specific complaints or request for issues of the client, who often complain, “I felt good for an hour, and then went back to normal.”
- Deep tissue therapists, mimicking a medical model, focusing solely on complaints, without a plan for integrating a whole body. This often results in a client walking out disorganized as the therapist plays hopscotch in isolated areas in what Tom Myers and others call “chasing pain.“ One financial drawback to this type of practice is that you only see clients when something is wrong rather than having the rewards of a large base of grateful regular clients and a consistently full practice.
I know countless very gratified and successful therapists who combine very pleasing full body massage while using specific skills of deep tissue massage on specific areas. Many clients long for a session that offers the benefits of relaxation while being a therapeutic part of a health maintenance program. These therapists consistently report a rewarding full practice of regular clients who love their work and refer to others.
This blog post article was created in collaboration with www.TerraRosa.com.au.
(Click here for a blog post article on Manual Therapy Certification for Massage Therapists.)
