Frictionless Theory
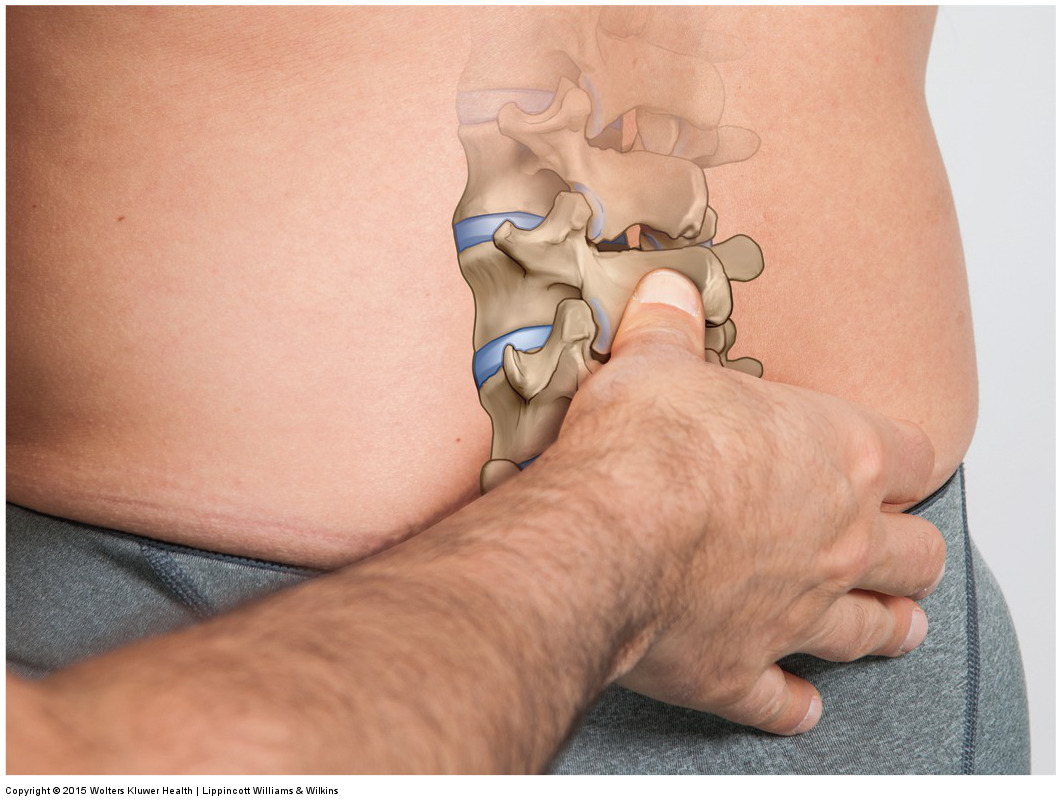
Lumbar joint mobilization. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
There is a “theory” that the skin-fascia interface with underlying bone is frictionless, and therefore only a perfectly perpendicular (90°, “compressive” / “normal”) force delivered during spinal manipulative therapy (SMT) can move the underlying vertebrae. If this theory is true, then it is essentially impossible to apply a force that is even slightly parallel with the surface of the bone (termed a shear force) that would have the ability to move the bone. In fact, if taken to its extreme interpretation, then even a force that is 89.9999° (.0001° off of perfectly 90° perpendicular) would be able to move/mobilize the target bone. This is extremely important to determine because joint hypomobilities are often in specific directions that are not necessarily perpendicular to the contour of the bone.
(Click here for another blog post article on Frictionless Theory and Manual Therapy.)
2009 Study
To test this hypothesis, researchers from Canada and USA, conducted a 2009 study using excised porcine lumbar spines (L3 and L4). SMP was applied using a compressed air device delivering force at 90° to the posterior tissues of the target vertebra; subsequently force was also applied at 60° and 120°. The resulting movement/mobilization of the vertebrae were recorded using an accelerometer.
Results
The results showed that vertebral movement was greatest at a 90° SMT application angle, as expected. However, although the movement was less, movement of the target vertebra did occur at directional angles other than perpendicular. In fact, the movement at the 60° and 120° angles was within 5% of the expected movement (when computed mathematically). This is important to emphasize because the frictionless theory, if carried to its extreme interpretation, would state that no movement at all would occur when any force other than a perfect perpendicular direction is applied.
The authors stated that this was done on a pig, and it is not yet known if variations in SMT application angle have relevance to clinical outcomes on human tissue. But that these findings should encourage future studies on human cadavers.
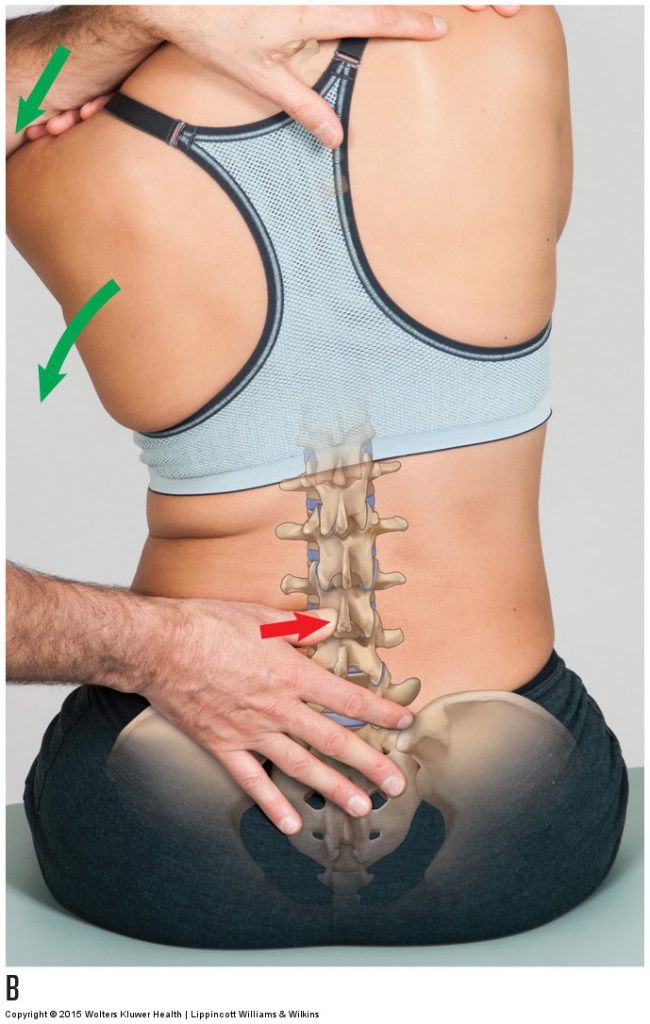
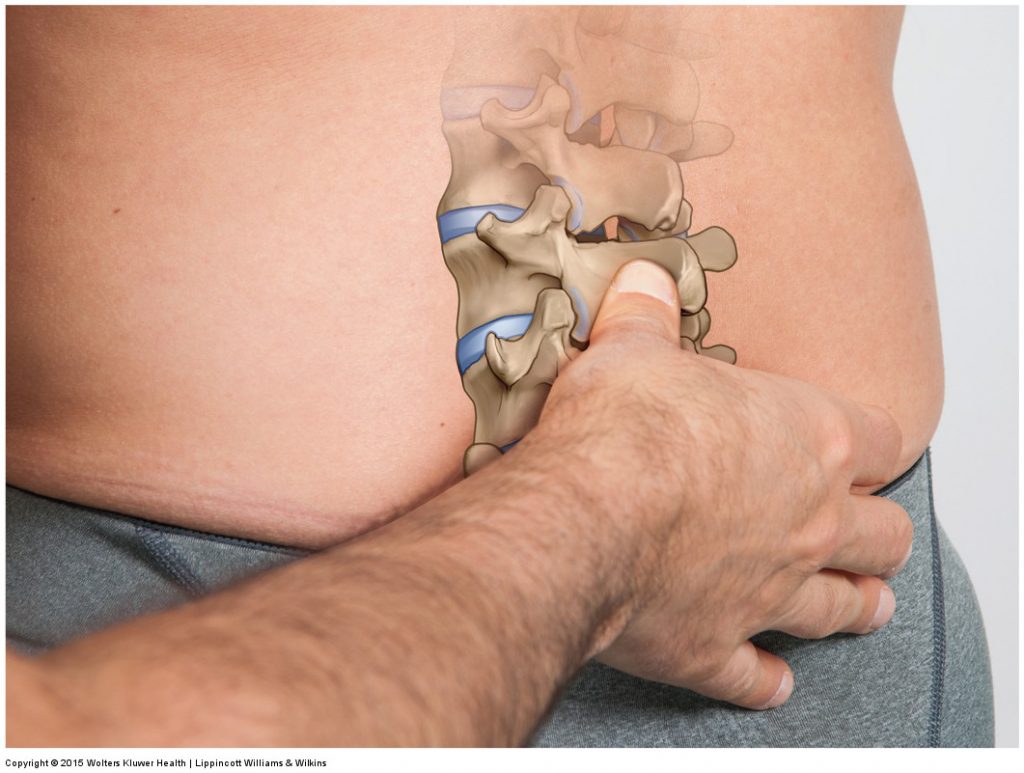
Mobilization of the lumbar spine. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Application
The application of this study is enormous. Many manual therapy professions employ joint mobilization techniques, whether they are slow oscillation Grade IV or fast thrust Grade V mobilizations. The ability to mobilize a joint is the ability to stretch and loosen its intrinsic fascial tissues, which is of extreme importance for all manual and movement therapy professions. After all, it could be said that the three major keys to musculoskeletal (or perhaps it should be stated neuro-myo-fascio-skeletal) health are strength of musculature, flexibility of soft tissues, and proper neural control. The implications of this study strike at the heart of increasing soft tissue flexibility.
Note:
There is some confusion regarding what the frictionless theory refers to when the “skin-fascia” interface is discussed. In a number of these studies that are referenced, the study is referring to the interface between the skin-fascia tissue (the superficial skin and subcutaneous fascia layer of tissue) and the underlying bone, in other words between the subcutaneous fascia and bone, NOT to the interface between the skin and subcutaneous fascia itself; so the term “skin-fascia interface” can be confusing because one could infer that it is the interface BETWEEN these two structures (skin and fascia) that is being referenced. Perhaps they should reference the name bone in the interface to make this clear. This is the case in the studies that discuss the ability of a manual therapist to move underlying bone (often done with reference to spinal manipulative therapy as the study discussed here does).
However, proponents of the frictionless theory also make reference to how it is also not possible to tension muscular tissue because of the frictionless nature of the interfaces between fascial layers themselves, in other words, between the subcutaneous fascia (of the skin-fascia tissue) and the fascia overlying/surrounding the muscles of the body (often termed deep fascia).
This blog post article was created in collaboration with www.TerraRosa.com.
(Click here for another blog post article on Frictionless Theory and Manual Therapy.)
