Manual therapy treatment for sacroiliac joint dysfunction
Sacroiliac joint dysfunction can involve a hypomobile joint or a hypermobile joint. The treatment for a hypomobile sacroiliac joint (SIJ) joint is Grade IV joint mobilization (also known as arthrofascial stretching). Note: Grade V joint mobilization should only be done if you are licensed to perform this technique. Joint mobilization treatment of the SIJ is identical to direct motion palpation assessment of the SIJ with the client/patient prone. But instead of pressing once or twice to determine the motion, sets of three to five oscillations should be done for treatment instead.
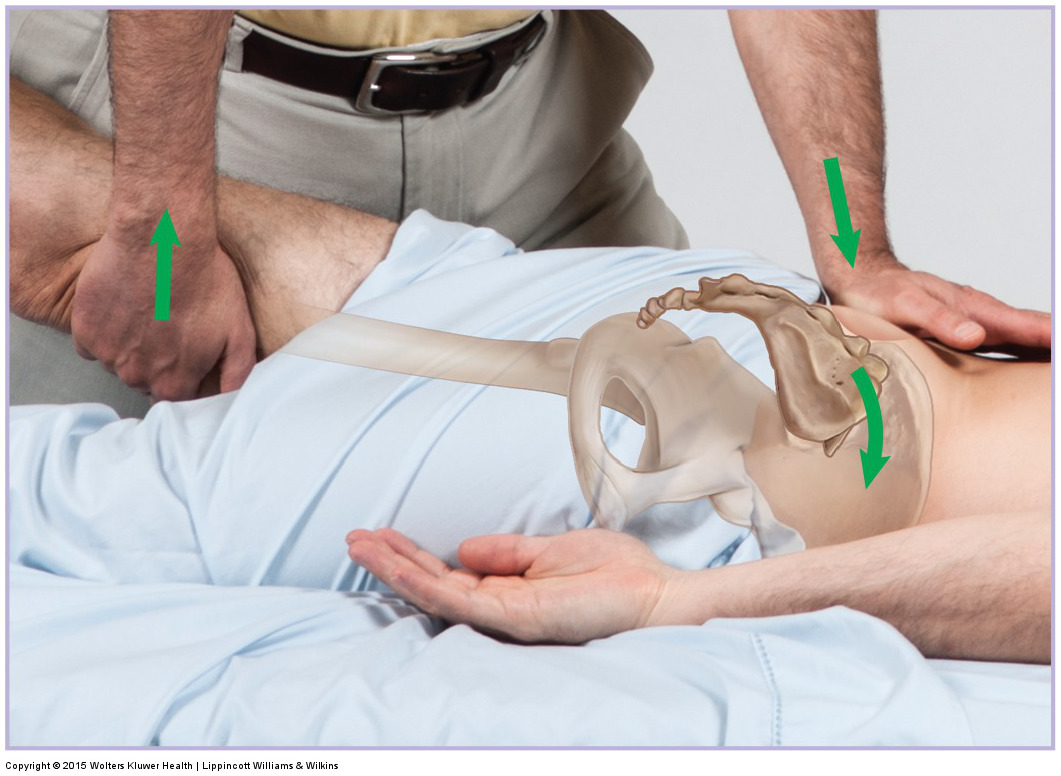
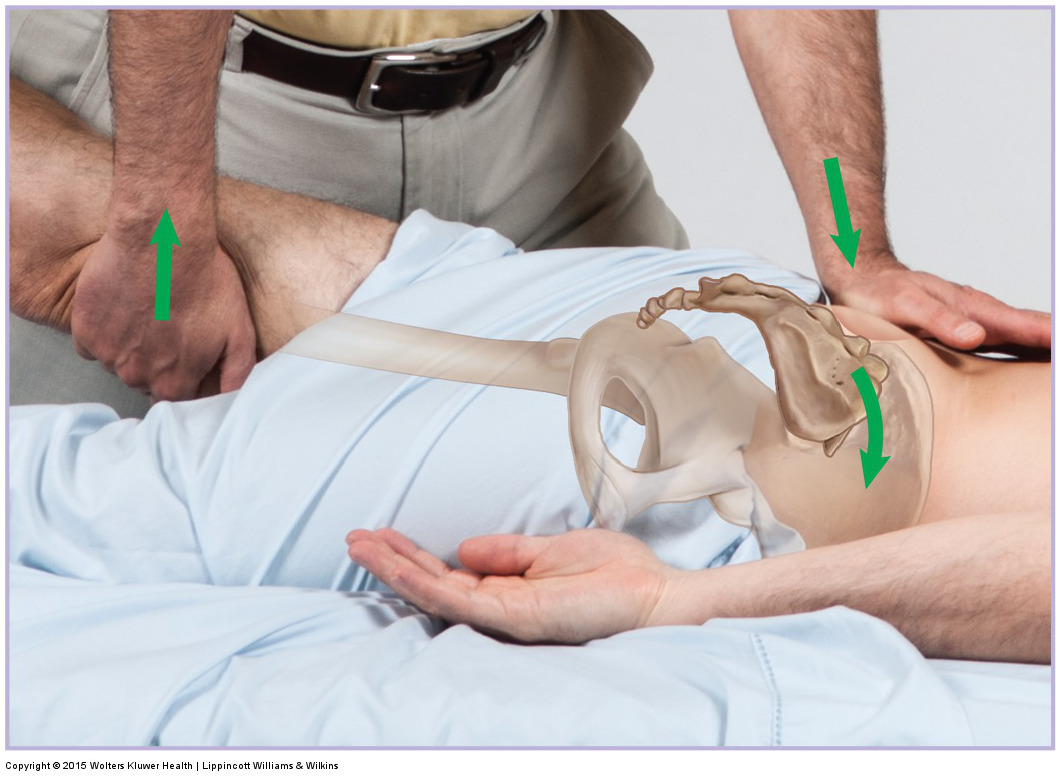
Joint mobilization of the sacrum into nutation (anterior tilt). Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
The force that is placed into the sacrum or pelvic bone should be gentle but firm, the movement should be slow, the bone should be moved an extremely small distance (literally an oscillating motion), and the end position of mobilization should be held for less than a second. This mobilization is usually repeated for a set of three to five oscillations; and anywhere from one to three sets of oscillations are usually done. Other practitioners recommend performing joint mobilization for a period of time instead, perhaps for 10, 15, or 20 seconds. As with all manual therapy techniques, the determinant for how long to apply a technique should be based on the response of the client’s/patient’s tissues.
The exact direction of pressure for the mobilization force should be dictated by the direction of hypomobility that was assessed with motion palpation. If the PSIS is being contacted and the force is toward anterior tilt of the pelvic bone, the mobilization force can be augmented by simultaneously lifting the client’s/patient’s thigh into extension.
It is extremely important to emphasize that a Grade IV mobilization should never involve a fast thrust. Implementing a fast thrust is defined as a Grade V manipulation and is usually only legal for Chiropractic and Osteopathic physicians.
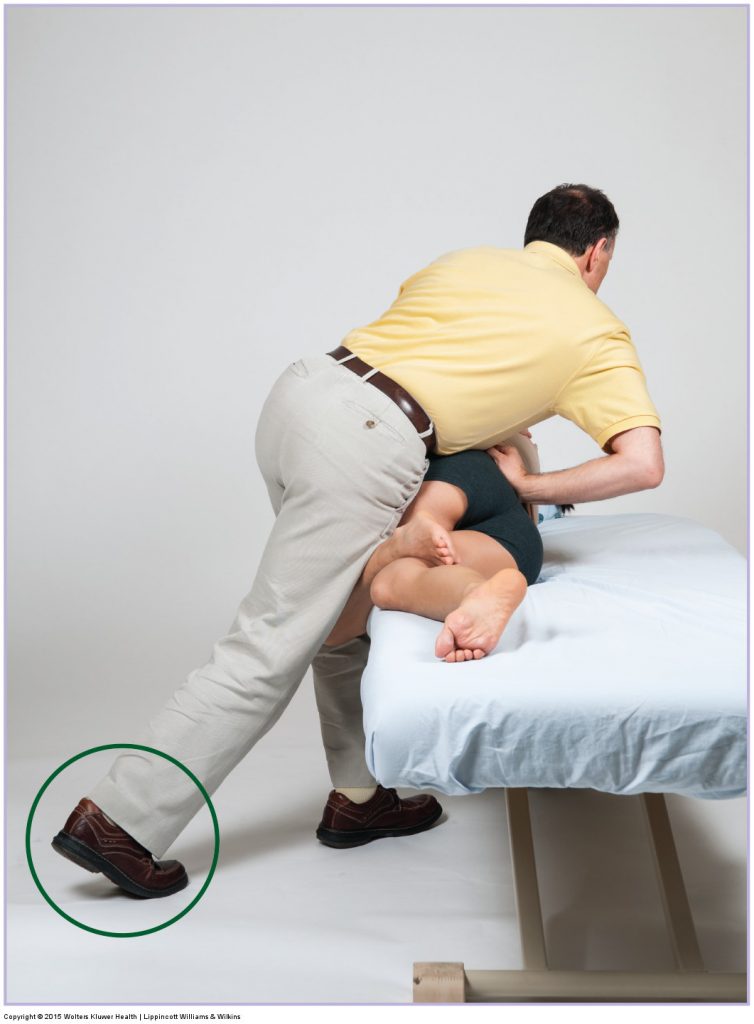
Side-lying joint mobilization for the sacroiliac joint. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Joint mobilization is most effectively performed after the area has first been warmed up. It should be done after moist heat, soft tissue manipulation, and regular stretching of the region has been done. These other techniques might also be helpful at removing muscular tightness and fascial adhesions that can be contributing to the restriction of motion that is part of the underlying problem. In particular, any stretch that is effective for the piriformis muscle will also be effective at stretching the SIJ.
If instead, the client/patient has hypermobility of the SIJ, then joint mobilization is not indicated, and in fact is contraindicated. Instead, assess the contralateral SIJ to see if it is hypomobile, causing the hypermobile SIJ as a compensation. Hypermobile joints are, by definition, unstable; therefore it is important to strengthen nearby musculature to increase stability. Specifically, the piriformis, gluteus maximus, and paraspinal musculature should be strengthened.
Because SIJ dysfunction typically causes no pain or decreased range of motion in the early to middle stages, clients often do not present for treatment until this condition is very chronic and progressed, and therefore stubborn and resistant to treatment. However, if consistent care is given, the condition can respond well to manual therapy. There are two aims of manual therapy for this condition. The first is to mobilize any and all hypomobilities. The second is to address any other conditions, including postural distortion patterns that the client/patient might have that are contributing to the joint dysfunction.
Summary of Manual Treatment Protocol for Sacroiliac Joint Dysfunction
| For Hypomobile Joint Dysfunction: |
| 1. Heat, soft tissue manipulation, and stretching of the associated musculature (specifically stretch the piriformis). |
| 2. Joint mobilization (arthrofascial stretching) |
| 3. Assessment and treatment of any concomitant condition that is contributing to the joint dysfunction. |
| 4. Counsel the client/patient regarding posture |
| For Hypermobile Joint Dysfunction: |
| 1. Treat contralateral SIJ if hypomobile (as indicated above) |
| 2. Assess and treat any concomitant condition that is contributing to the joint dysfunction. |
| 3. Counsel the client/patient regarding posture |
| 4. Strengthen the associated musculature to increase stability |
Precautions/contraindications for sacroiliac joint dysfunction
Joint mobilization is a very powerful technique; therefore it should always be performed with caution. Joint mobilization is contraindicated if the physical integrity of the client’s/patient’s spinal tissues is compromised, in other words, there is an acute sprain, strain, or osseous facture. Joint mobilization is also contraindicated if a joint is hypermobile. If the apex of the sacrum is being contacted to mobilize the sacrum toward posterior tilt (counter nutation), be sure to not press on the coccyx. This could injure the sacrococcygeal ligament.
