Manual therapy case study for sciatica
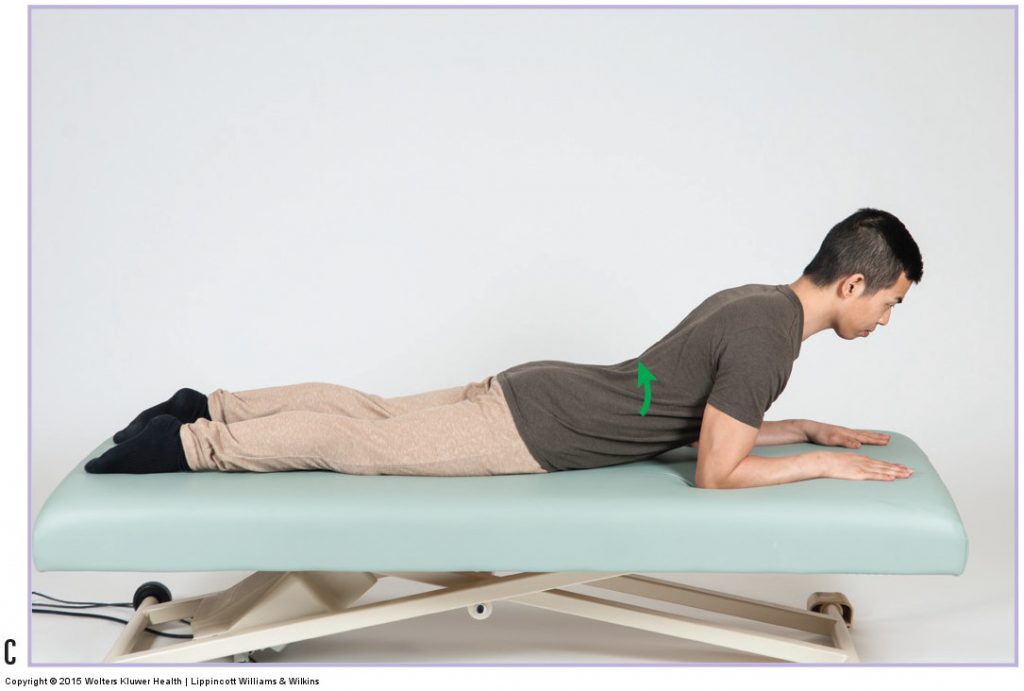
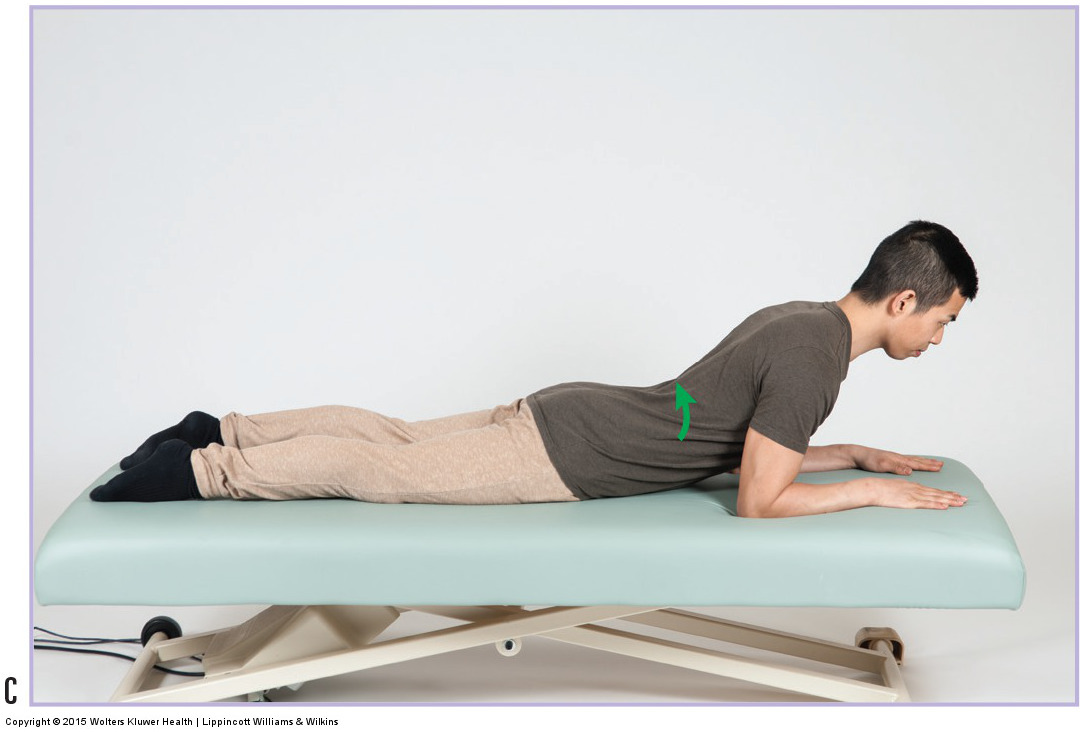
Stretching exercise of the spine into extension. Permission: Joseph E. Muscolino. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Armin is a 35-year-old office manager who has noticed a burning pain at the outside of his left leg. The pain began insidiously approximately four weeks ago. At first it was barely perceptible, but it has gradually worsened and is now quite uncomfortable. He notices that it tends to be worse on weekdays when he spends more time sitting. Armin has decided to consult an orthopedic manual therapist to see if massage could help.
The therapist performed passive straight leg raise (SLR), slump test, cough test and Valsalva maneuver. Armin was negative for referral to cough and Valsalva, but SLR and slump test did reproduce the typical referral pattern that he has been experiencing. Armin’s lumbar paraspinal musculature (erector spinae and transversospinalis / multifidus) and quadratus lumborum are markedly tight bilaterally and all lumbar spinal ranges of motion are decreased. His piriformis muscles are mildly tight but not tender to palpation; and his hip joint ranges of motion are within normal limits.
Given that Armin has been experiencing burning pain in the lateral leg which is typical of sciatica, it seemed fairly certain that he was experiencing sciatica. What the therapist had to determine was the cause or causes. Positive SLR and slump indicate a space-occupying (nerve compression) lesion, most likely due to a pathologic disc or bone spur. However, because cough and Valsalva are negative, the space-occupying lesion does not seem to be markedly severe. None-the-less, reproduction of Armin’s lower extremity referral pain with SLR and slump test are strong enough indicators that the therapist decided to refer Armin to a local physiatrist for a more definitive workup.
But because the therapist also found Armin’s lumbar musculature to be markedly tight, he recommended that Armin come in twice a week for three weeks to work on this musculature because it might be contributing to the sciatica by compressing the IVFs and disc joints. Therefore, loosening the paraspinal muscles would be beneficial.
The therapist’s session consisted of moist heat, soft tissue manipulation, and stretching to the low back with double knee to chest stretch performed with agonist contract technique and stretching the left side of the low back with Armin side-lying on his right side and his right left lower extremity dropped off the side of the table behind him. This was followed by moderate depth pressure soft tissue manipulation to Armin’s gluteal regions and hamstrings bilaterally, and also contract relax (CR) (also known as PIR or PNF) stretching to the hamstrings bilaterally. For self-care, the therapist recommended that Armin gently stretch his lumbar region with double knee to chest stretch. She also recommended that Armin avoid sitting as much as possible, and that he start extension (McKenzie) exercises to build up the strength of his low back.
The physiatrist ordered an MRI and found that Armin has a mild disc bulge in his lower lumbar spine. The physiatrist recommended a Medrol dose pack of steroidal anti-inflammatory medication and rest, and to return if his symptoms had not improved.
At the end of three weeks, Armin’s lower extremity symptoms were relieved and his low back musculature was markedly looser. The therapist progressively weaned Armin down to one visit every two to four weeks for proactive care.
