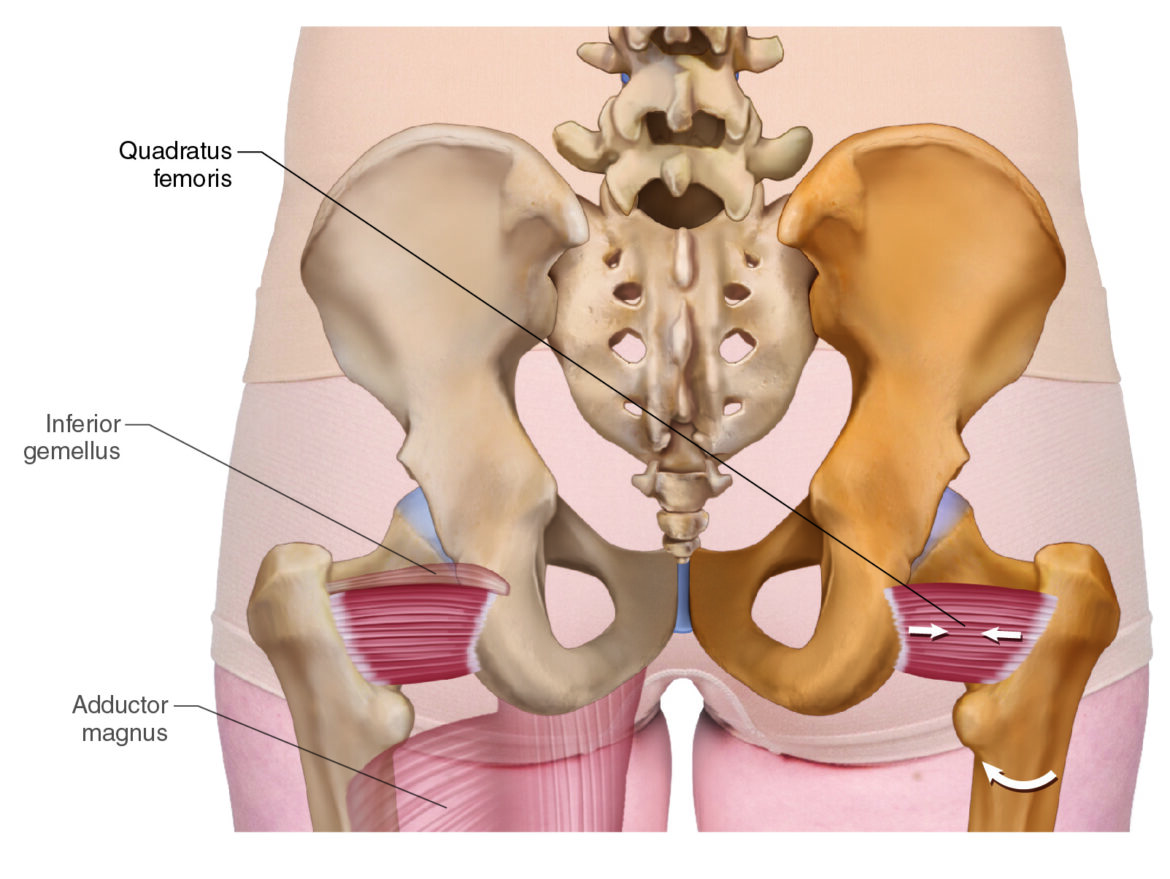
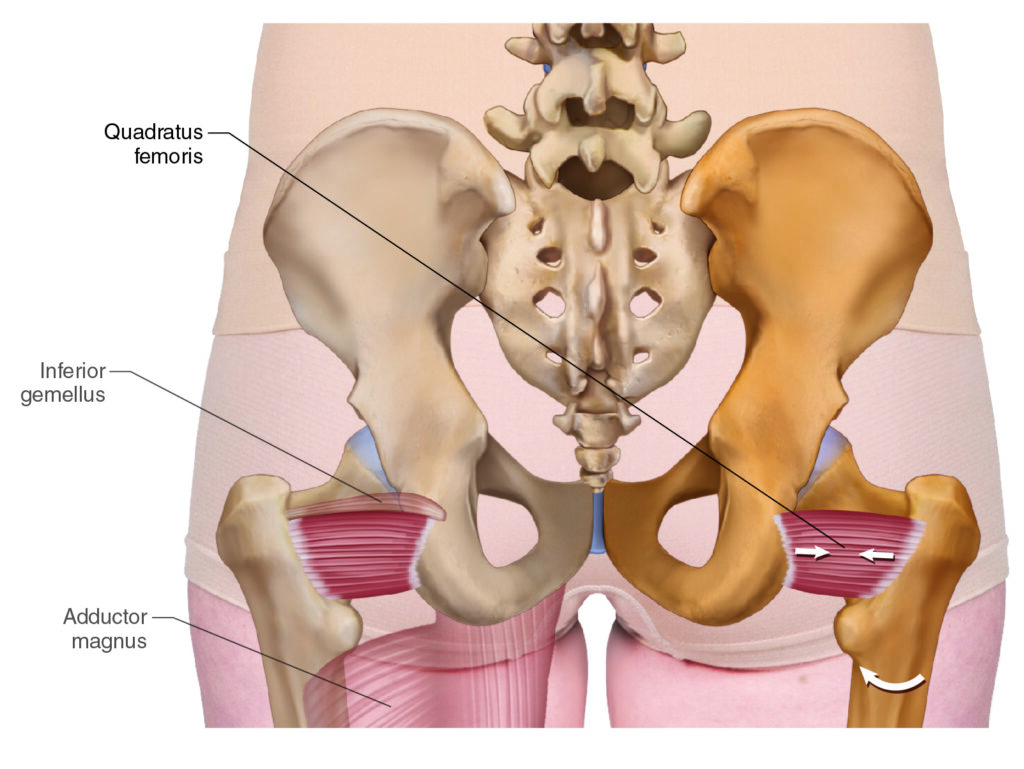
Quadratus Femoris. Permission Dr. Joe Muscolino (learnmuscles.com)
Introduction
The quadratus femoris (QF) is one of the six muscles in the deep lateral rotator group. It is the most inferior of the six, and usually the largest, even though the piriformis is usually the most well-known of the group. When a client presents with pain in the gluteal region, the piriformis might be the usual suspect, but the cause of their pain may well be caused by an unusual suspect, the QF.
Quadratus Femoris Attachments
The QF attaches proximally from the ischial tuberosity (origin) to distally on the femur (insertion).
More specifically, it attaches from the
- lateral border of the ischial tuberosity
to the
- intertrochanteric crest of the femur
The Deep Lateral Rotator Group
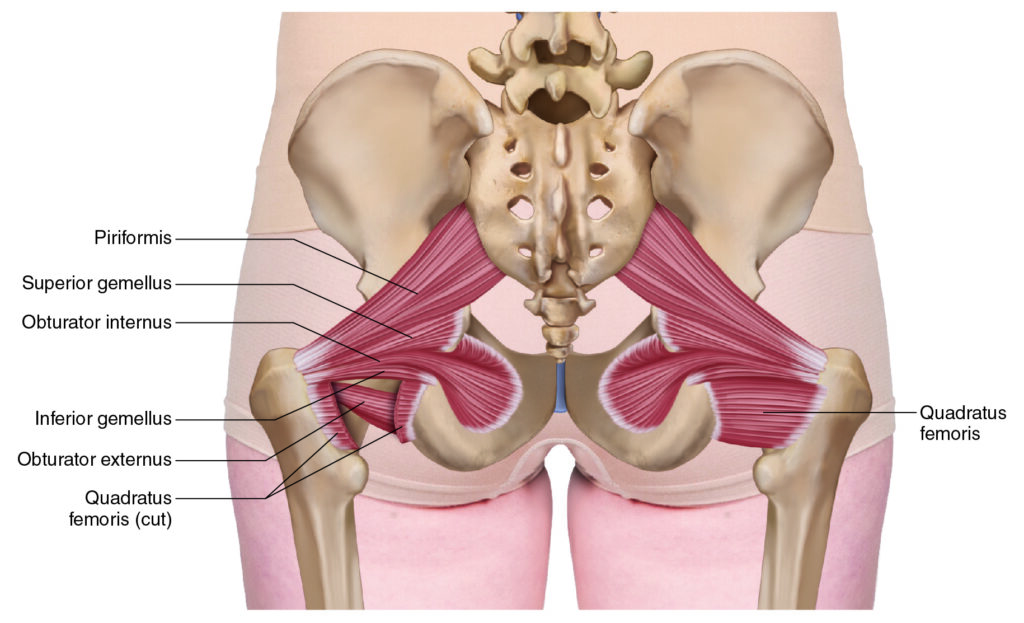
The Deep Lateral Rotator group. Permission Dr. Joe Muscolino (learnmuscles.com)
The QF is one of the six muscles in what is called the deep lateral rotator group. They are so-named because they lie deep in the gluteal region (deep to the gluteus maximus) and all do lateral rotation (of the thigh at the hip joint).
The six muscles in the group are, from superior to inferior…
- Piriformis
- Superior gemellus
- Obturator internus
- Inferior gemellus
- Obturator externus
- Quadratus femoris
The QF is what I like to call a Rodney Dangerfield muscle because it does not get enough respect (this is based on the comedian from years ago named Rodney Dangerfield whose constant schtick was that he did not get enough respect). Because the QF is the same group as the piriformis, the piriformis gets all the attention, so the QF is often overlooked.
Note: To a great degree, the piriformis does deserve a lot of respect, and perhaps the most respect in this group, because in addition to being a lateral rotator of the hip joint, it also has a role in stabilization of the sacroiliac joint. Having said this, it does not mean that the piriformis is the causitive pathomechanism in every client who presents with gluteal pain.
Quadratus Femoris Functions
Open-Chain and Closed-Chain Functions
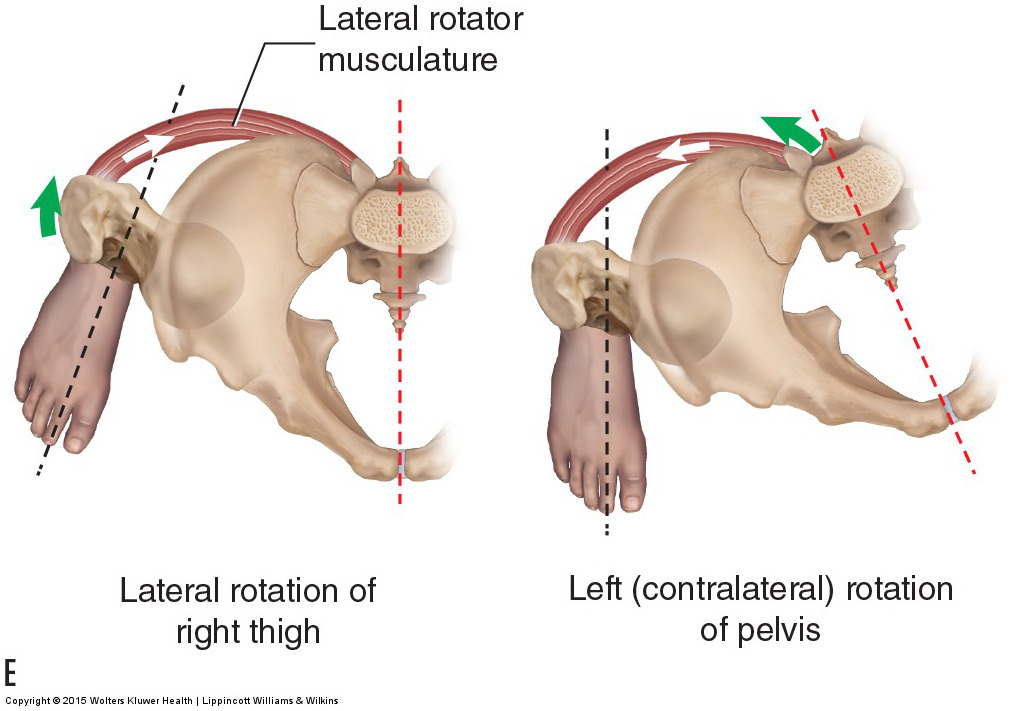
Open-chain lateral thigh rotation and closed-chain contralateral pelvic rotation at the hip joint. Permission Dr. Joe Muscolino (learnmuscles.com)
Open-Chain Function
The QF crosses the hip joint posteriorly, running horizontally from medial to lateral, so in open-chain, it pulls the femoral attachment toward the pelvic attachment, resulting in lateral rotation of the thigh at the hip joint (as the name of the group implies).
And, because it lies below the center of the hip joint, it can also assist with adduction of the thigh at the hip joint.
And… if the thigh is first flexed to 90 degrees, the QF can horizontally abduct the thigh at the hip joint.
Closed-Chain Function
Closed-chain, it pulls the pelvic bone toward the femur, resulting in contralateral (opposite-side) rotation of the pelvis at the hip joint.
| Chain | Action |
|---|---|
| Open-chain | Lateral rotation of the thigh |
| Open-chain | Assists adduction of the thigh |
| Open-chain (thigh flexed 90°) | Horizontal abduction of the thigh |
| Closed-chain | Contralateral rotation of the pelvis |
Nearby Anatomy
Posterior views. Superficial on the left; deep on the right. Permission Dr. Joe Muscolino (learnmuscles.com)
As we have said, the QF is the most inferior member of the deep lateral rotator group; therefore, it lies deep to the gluteus maximus. The inferior gemellus is directly superior, and the obturator externus actually lies in an even deeper layer, deep to the QF from the posterior perspective. Given that the QF attaches onto the ischial tuberosity, it lies close to the adductor magnus and the hamstring group musculature. On the other (medial) side of the ischial tuberosity is the coccygeus and levator ani of pelvic floor musculature.
For a thorough atlas of musculoskeletal high-resolution images that you can download and use in your teaching, click here.
Palpating the Quadratus Femoris

Palpation of the quadratus femoris. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual, 3rd ed.
The QF is actually quite easy to palpate. Have the client prone with their (lower) leg flexed 90 degrees at the knee joint. Place one hand contacting on their distal medial leg, just proximal to the ankle joint. With your (other) palpating hand (with verbal consent of the client), find the inferior aspect of the ischial tuberosity, and then palpate laterally and superiorly along the ischial tuberosity until you can feel the vertical lateral border. Drop immediately lateral off the lateral border and you will be on the QF (deep to the gluteus maximus). Now ask the client to try to laterally rotate their thigh at the hip joint against your resistance with your contact on their distal leg, and you should feel the QF pop. Palpate the entirety of the QF as you ask the client to alternately contract and relax it.
Once you have located the QF, have the client fully relax it and palpate for any tightness/tautness, whether it is global hypertonicity, focal myofascial trigger points (TrPs), and/or fascial adhesions.
Stretching the Quadratus Femoris
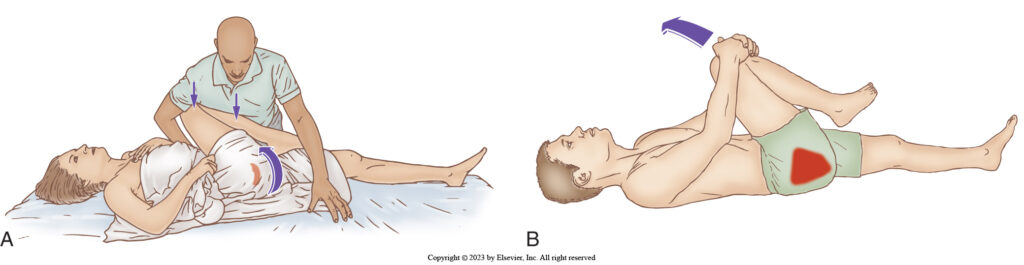
Stretching the QF with horizontal adduction: therapist-assisted and client self-care. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual, 3rd ed.
The QF is stretched in the same manner as the piriformis. With the client prone, it can be stretched with medial rotation of the thigh at the hip joint (given it is a lateral rotator). However, a precaution is that because this method uses the (lower) leg as a lever to create the femoral rotation, it places a torque into the knee joint. If the client’s knee joint is unhealthy, this method is contraindicated.
Another palpation protocol (see above) is to have the client supine and stretch the QF with horizontal adduction of the thigh at the hip joint (given it is a horizontal abductor). This is also the same protocol as stretching the piriformis, except that the angle to the stretch force is a bit different; orient their thigh more superiorly to preferentially focus the stretch on the QF (versus the piriformis).
And remember that stretching is always safer and more effective if the client’s tissues have first been warmed up.
Massaging the Quadratus Femoris
The sciatic nerve. Permission Dr. Joe Muscolino (learnmuscles.com).
The QF responds quite well to heat and massage, followed by stretching. Regarding massage, it can be worked with vertical (cross-fiber) and/or horizontal (longitudinal) strokes. One precaution that therapist should be aware of when palpating and massaging the QF is that the sciatic nerve travels superficially over its medial aspect, directly next to the ischial tuberosity.
Case Study – The Unusual Suspect
The presence and importance of the QF was made clear to me many years ago when a patient presented to me with pain in her gluteal region. My first thought was that it would be the piriformis, but upon careful palpation assessment of the piriformis, I did not find any densification of tissue, and she indicated that the pain was more inferior. I kept palpating the musculature of the deep lateral rotator group, until I reached the QF, far inferior, between the ischial tuberosity and femur. Once I reached the QF, I could feel a clearly palpable myofascial trigger point (TrP), and upon digital pressure, the patient reported that it reproduced the same pain that she had been experiencing.
In her particular case, because she came in literally the day after the pain had begun, one treatment sufficed to eliminate the TrP and her pain. A note here… it is usually not the severity, but rather the chronicity (i.e., how long the client has had the problem) that determines how much treatment is necessary to help resolve the client’s condition. This is because with chronicity, neural facilitation (muscle memory) entrenches the hypertonicity, the continued tightness perpetuates any TrPs and often results in secondary TrPs, and fascial adhesions build up. In this case, because she came in so quickly, the case resolved quickly.
The biggest take-home for me after working with this patient was to not always assume that the client’s pain and/or dysfunction is caused by the usual suspect(s)… in this region, the piriformis. Therapists often like their favorite muscle in the region to be the one they assess as causing the client’s problem. But, fairly often, it is another unusual suspect that might be the cause. But we will not find it unless we look for it! And even if our favorite/usual suspect muscle is found to be tight, we should keep looking and assess all the myofascial tissues in the area. One hypertonic muscle often results in compensatory tightness in other nearby muscles. We should always palpate and assess every inch of the suspected region before completing our assessment.
Conclusion
As mentioned in the case study above, we need to be thorough in our assessment of the client. Never assume that their problem is only coming from the usual suspect(s) in the area. In the case of the gluteal region, most every therapist is familiar with the piriformis, but it can be crucially important to also be aware of, and competent assessing and treating, the quadratus femoris (QF) as well!
Frequently Asked Questions About the Quadratus Femoris
- What is the quadratus femoris?
- The quadratus femoris (QF) is one of the six muscles in the deep lateral rotator group. It is the most inferior and usually the largest of the six, lying deep to the gluteus maximus in the gluteal region.
- Where does the quadratus femoris attach?
- The QF attaches proximally from the lateral border of the ischial tuberosity to distally on the intertrochanteric crest of the femur.
- What muscles make up the deep lateral rotator group?
- The six muscles are (superior to inferior): piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and quadratus femoris.
- What are the functions of the quadratus femoris?
- In open-chain: lateral rotation of the thigh at the hip joint, assists with adduction, and (thigh at 90°) horizontal abduction. In closed-chain: contralateral rotation of the pelvis at the hip joint.
- Can the quadratus femoris cause gluteal pain?
- Yes. Myofascial trigger points (TrPs) in the QF can reproduce gluteal pain that is often mistakenly attributed to the piriformis. Thorough palpation of all deep lateral rotator group muscles is essential for accurate assessment.
- How is the quadratus femoris treated?
- The QF responds well to heat and massage (cross-fiber and longitudinal strokes), followed by stretching. Stretching is performed with medial rotation of the thigh (prone) or horizontal adduction (supine), with precautions for clients with knee joint issues.

Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com.
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
