Postoperative Abdominal Adhesions
Abdominal Adhesions
Postoperative abdominal adhesions are pathological adhesions that develop between abdominopelvic structures following surgery. Considered unavoidable and ubiquitous, postoperative adhesions can lead to bowel obstructions, infertility, pain, and the need for further operations. As such, they represent a substantial health care challenge. Despite over a century of research, no preventive treatment exists. Visceral manipulation has been promoted to address this adhesion problem, however the evidence of its efficacy is still scarce.
Research Study with Manual Therapy
In an article published in the open access journal Plos One, authors Geoff Bove from University of New England College of Osteopathic Medicine, and massage therapist Susan Chapelle, and colleagues, conducted an experiment to test the hypothesis that postoperative adhesions develop from a lack of movement of the abdominopelvic organs in the immediate postoperative period when the patient is immobile from rest and opiates. The authors further tested whether manual therapy would prevent their development. Rat models were used to test their hypothesis.
This study used 147 rats that were operated upon to induce adhesions, and assigned to receive either treatment or remain untreated. Their resulting adhesions were quantified. They also evaluated the type and number of macrophages that were formed (macrophages are a type of white blood cell that is formed in response to an infection or accumulated damaged or dead cells).
In separate experiments, they also tested the effect of manual therapy for adhesions formed from two surgical treatments of adhesions: strictureplasty (surgery to alleviate bowel narrowing due to scar tissue), and adhesiolysis (surgery to remove or separate adhesions).
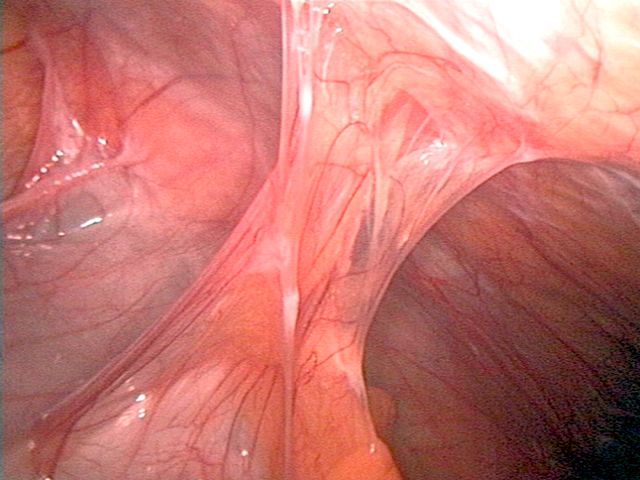
The experiment shows that following surgery, adhesions between the cecum and abdominal wall were found. In addition, adhesions were also commonly found between the greater omentum and cecum, and between adnexal fat pads and cecum. Adhesions connecting intestine to intestine (an example of a cohesive adhesion) were not often found in all rats, but when they occurred they were flat, rather than band-like.
Results
The results showed that the manual treatment leads to smaller and less frequent abdominal adhesions between the cecum and the abdominal wall; but manual treatment had no detectable effect on abdominal adhesions involving the greater omentum or adnexal fat pads. Other cohesive and band-like abdominal adhesions were not prevalent enough in this study to be reliably measured for a difference between the treatment and control groups. The researchers assumed that this lack of response is due to the inability to accurately palpate those structures.
The authors suggest that although the treatment was on rats, it is likely that these manual therapy treatments would induce similar sliding motions between structures in humans. A concern about mobilization immediately after surgery is that it could disrupt delicate sutures. However, the results show that in freely mobile surgeries (strictureplasties) that even very fine sutures were not disrupted by treatment directed to the repair site, and therefore healing was not impaired.
The authors hypothesised the primary mechanism of action of visceral manipulation could be quite simple. Peritoneal damage leads to fibrin secretion, and fibrin is an adhesive. Postoperative ileus may act like a clamp and thus allow the fibrin glue to “set.” The movement induced by manual treatment may simply keep the structures moving enough to prevent these adhesions from adhering until normal peristalsis resumes and fibrinolysis (breakdown of clots) becomes dominant.
This study demonstrates that manual therapy initiated immediately postoperatively is an effective preventive approach for postoperative abdominal adhesions.
The techniques of visceral manipulation are not complex and can be used to safely mobilize the postoperative abdomen. While there is a compelling possible mechanism that relates to the reduction in macrophage formation, it seems more likely that the primary beneficial mechanism is the maintenance of relative motion between healing surfaces.
It should be added that if this is the case, it might be possible that motility of the gut created by other means, such as with tolerable prokinetic drugs or early ambulation, may also result in the reduction of adhesion formation.
Note: This blog post article was created in collaboration with TerraRosa.com.au.
(Click here for another blog post article on fascial adhesions.)
