
Do and Don’t Precautions

Massage stroke over the thoracic region. Permission Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck (Elsevier, 2013).
This is the second list of miscellaneous, somewhat random, do and don’t precautions that I believe would improve massage therapy sessions with clients. I am not sure that everyone would agree with all of these precautions, but I offer them for consideration anyway. I would say that if you agree with any of them, you can bet that many of your clients will as well. The problem is that often a client will not want to criticize what the massage therapist does. It is easier for the client to simply smile and say that the session was good, and then never return. This is pity, especially when it might be because of a few small things that could easily be changed.
So, I offer the following massage therapy do and don’t precautions for your consideration. Who knows, it any of these improve your clients’ experiences, then it will probably improve your business as well! ?
Precaution #1: Do let the client breathe between strokes over the thoracic rib cage region
It is always nice to find a rhythm between the application of our massage strokes and the client’s breathing. However, when working on the thoracic rib cage region with the client prone, it is absolutely necessary. Breathing in requires the rib cage to expand anteriorly to posteriorly (as well as laterally), so if the therapist is pushing down on the client’s thoracic region as the client is trying to breathe in, it can be very uncomfortable for the client because their rib cage is expanding upward as the therapist is pushing down on it. This needn’t be a problem if we coordinate our strokes with the client’s breathing. Perhaps this precaution will not become an issue because the rhythm of the breathing will happen naturally, but if it doesn’t, then we can simply talk with the client. We ask them to breathe in, and then when they are breathing out, we sink in with our strokes. Depending on how long their breath out it, and depending on the length and speed of our strokes, we can usually perform between one and three strokes before we ease off and allow them to breathe in again. It is also usually helpful for us to coordinate our breathing with the client’s breathing, so when the client breathes in, we breathe in with them; when they breathe out, we breathe out with them.
Precaution #2: Do sink in slowly when using deep pressure
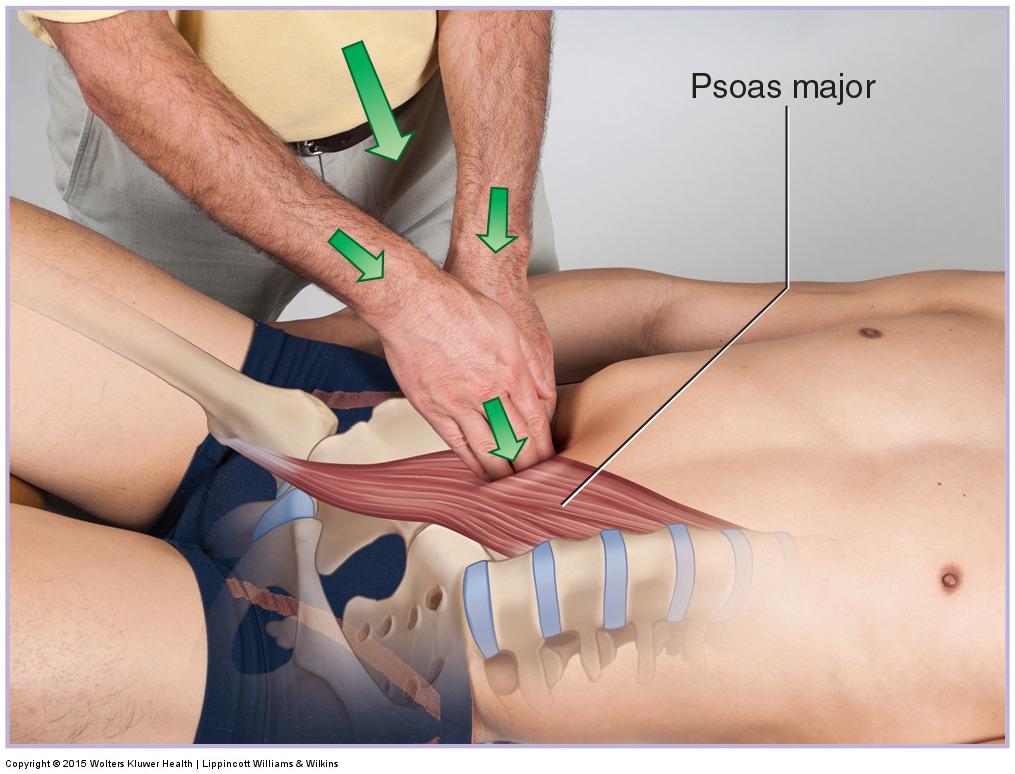
Deep pressure into the psoas major abdominal belly by sinking in slowly! Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (Elsevier, 2015).
This precaution is extremely important. Deep pressure is not always wanted or needed, but when it is appropriate to apply, it is amazing how much depth we can employ with the client remaining comfortable… if we apply our force slowly. Quick pressure tends to make the client reflexively respond by pushing back and fighting our work. But going slowly allows them time to relax and allow us to gradually increase our force into their tissues. I like to describe our application of the pressure as “sinking” into the tissues.
Precaution #3: Don’t let the client hold their breath out when we are applying deep pressure or stretching them
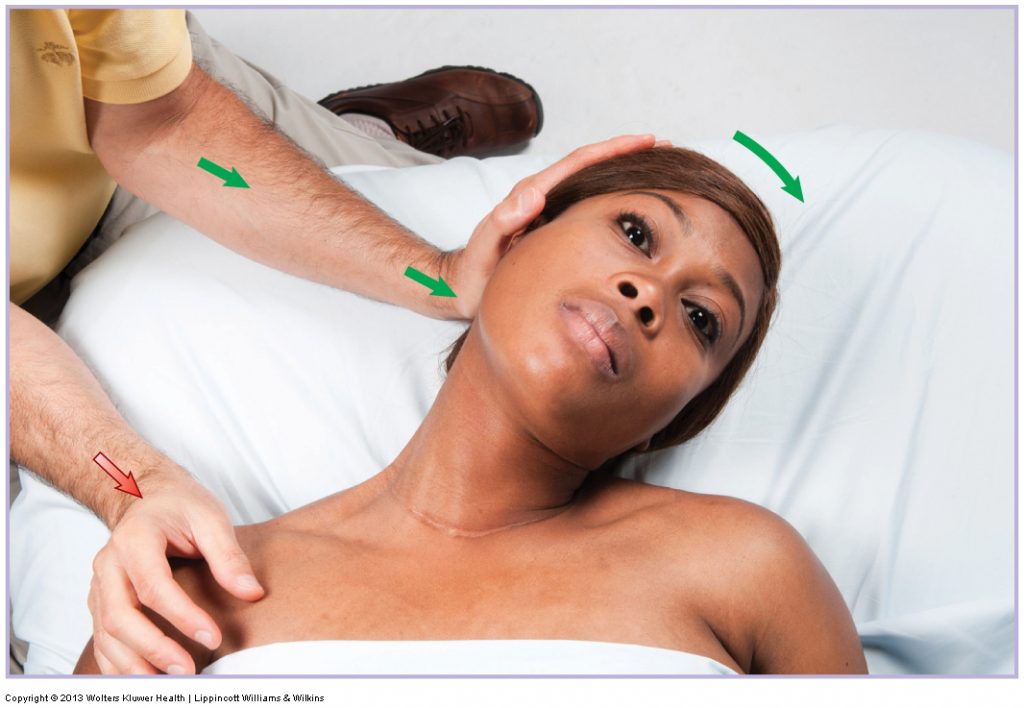
When stretching the client, have them breathe with you as you apply the stretch. Permission Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck (Elsevier, 2013).
As mentioned in Point #1 above, working with the client’s breathing is always a good idea, but is quite necessary when working the thoracic region. It is also effectively necessary when applying deep pressure or stretching the client. For the client to accept deep pressure or a stretch, they need to be relaxed, and people are usually most relaxed when breathing out. So don’t let them hold their breath, which is something that many people instinctively do when they feel as if they will experience pain. The problem is that holding their breath in tends to make their body rigid, which results in our pressure feeling rigid too, and therefore, painful. So we need to ask them to breathe in; and then as they breathe out, we breathe out with them, slowly sinking into their tissues, gradually increasing the depth of our pressure into their tissues or applying the stretch (or joint mobilization force for that matter). Although finding a rhythm to breathing when doing massage is fairly straight forward, there is often considerable controversy / confusion when performing stretching, especially neural inhibition stretching techniques such as CR / PIR /AC / PNF (i.e., contract relax, post-isometric relaxation, agonist contract, proprioceptive neuromuscular facilitation). In my opinion, the only imperative precaution rule regarding stretching and breathing is that the client should be breathing out when we apply the actual stretch force, because when breathing out they will be relaxed and allow a comfortable and effective stretch.
Precaution #4: Don’t lead with the fingertips…
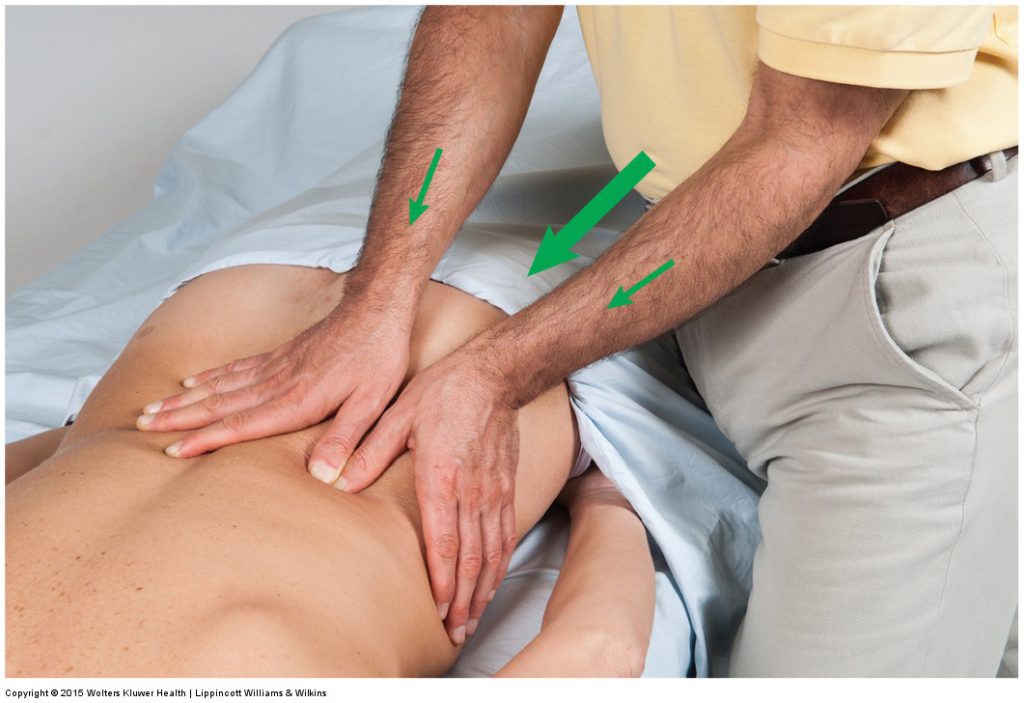
Don’t lead with the finger/thumb tips! Work with the pads of the thumbs/fingers. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (Elsevier, 2015).
We have a choice of many contacts when working on our clients. These contacts range from small to large. Small contacts are the thumb or fingers; large contacts are the elbow or forearm; and other contacts such as the flat palm, ulnar side of the hand, or fist are in between in size. The advantage to smaller contacts like the thumb or fingers is that they tend to be more sensitive for our palpation assessment and more specific for the force being applied while we are working. The disadvantages are that they are relatively fragile contacts that can be injured with overuse and that they tend to be “pokey” and uncomfortable for the client. So, this precaution is that when we do need to use the thumb or fingers, it is a good guideline to always try to contact the client with the pad of the thumb or fingers, instead of the tips of the fingers. In other words, do not lead with the fingertips. Certainly there are a few cases where we have no choice but to lead with the thumb/fingertips, such as accessing the quadratus lumborum or rib attachment of the anterior or middle scalenes. But other than a handful of these exceptions, we should always try to use the pads instead of the tips. One note of caution: We do not need to or want to work with the totally flat part of the pad of the thumb or fingers because this would compromise our body mechanics, either requiring such a shallow angle of force that we cannot generate any depth of pressure, or requiring us to torque or hyperextend the joints of the thumb or other fingers. It is only necessary to flatten out sufficiently so as not to be pokey or uncomfortable for the client.
Precaution #5: Don’t pull hairs!
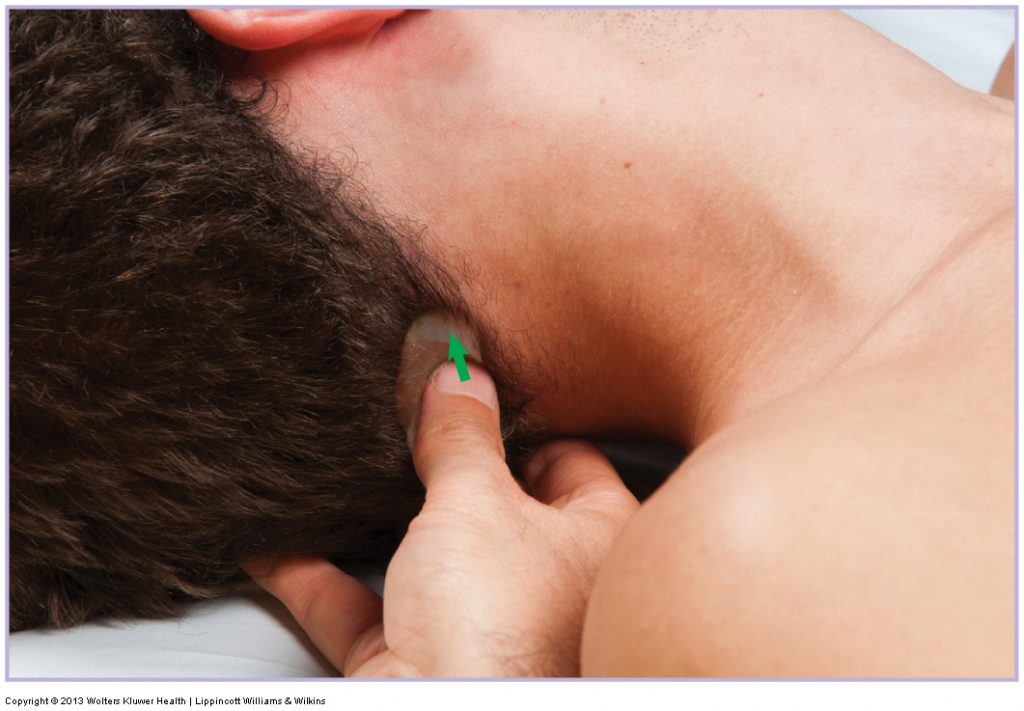
Do not pull hairs when working on the client! Permission Joseph E. Muscolino. Advanced Treatment Techniques for the Manual Therapist: Neck (Elsevier, 2013).
I love deep pressure when receiving massage, but if you pull any of the hairs on my body, I will cry like a baby! And I am not the only one who feels this way. Pulling hairs can occur anywhere that the client is hairy on their body, but can be especially problematic on the pectoral/chest region and the suboccipital region at the hairline. So precaution should be observed when working in these areas. One way to prevent hairs being pulled is to use more lotion. Of course, the more lotion that is used, the harder it is to generate deep pressure because the point of lotion is slide along the skin, so excessive lotion causes us to slide along the skin instead of sinking down into the tissues. So the appropriate amount of lotion needs to be used, which is the minimum amount necessary to not abrade the skin AND not pulls hairs. Another way to avoid pulling hairs is to instead work with a towel on the client’s skin; we then use the towel to grab the skin and move the skin and subcutaneous fascia over the underlying musculature, in other words, friction massage. And of course, static compression would be another way to avoid pulling hairs given that we are not moving along the client’s skin. Whichever way you choose to go, when you have a client that has a lot of body hair, please be careful so that you don’t pull their hairs.
(Click here for the blog post article: Ten Massage Therapy Dos and Don’ts.)
