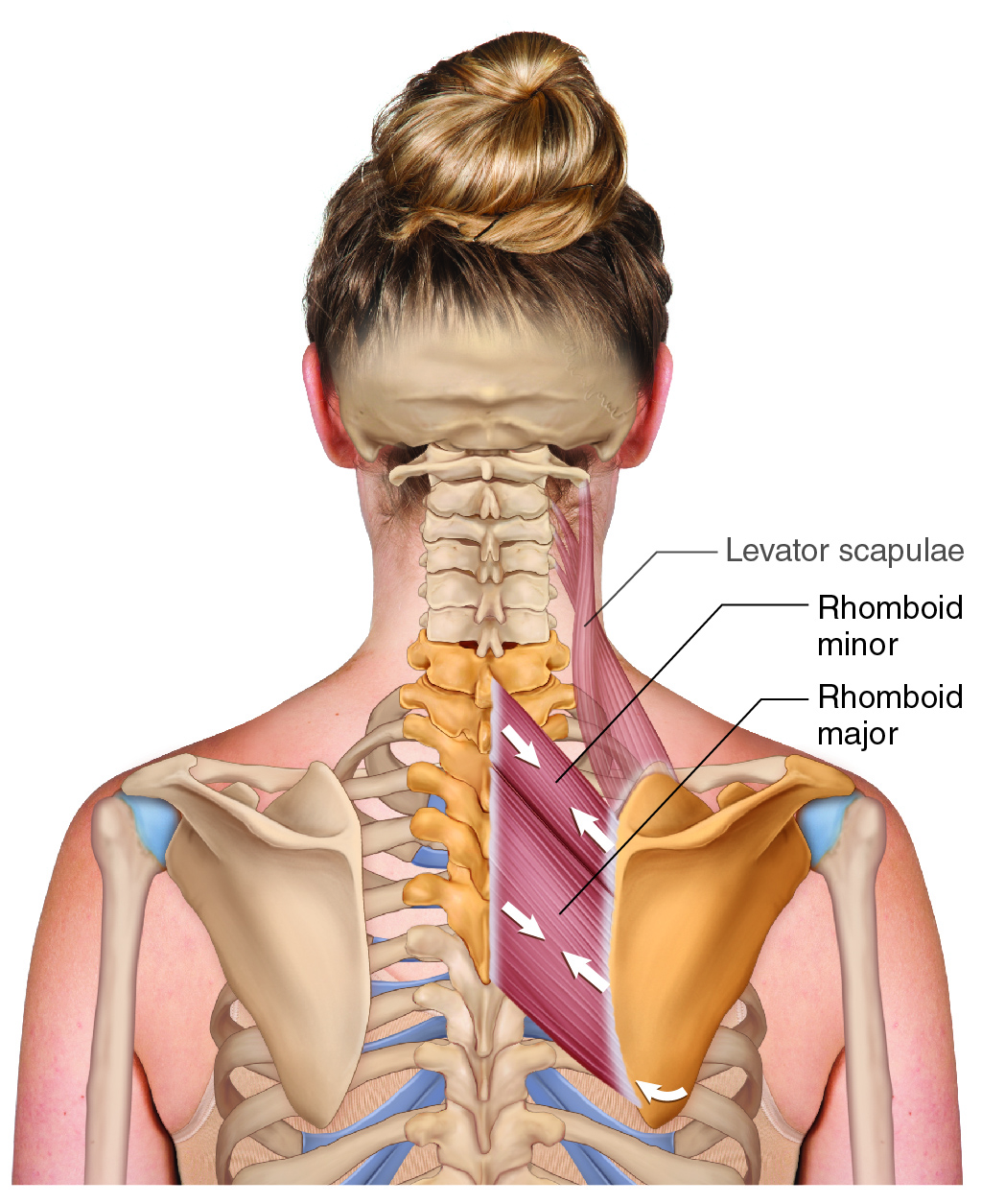
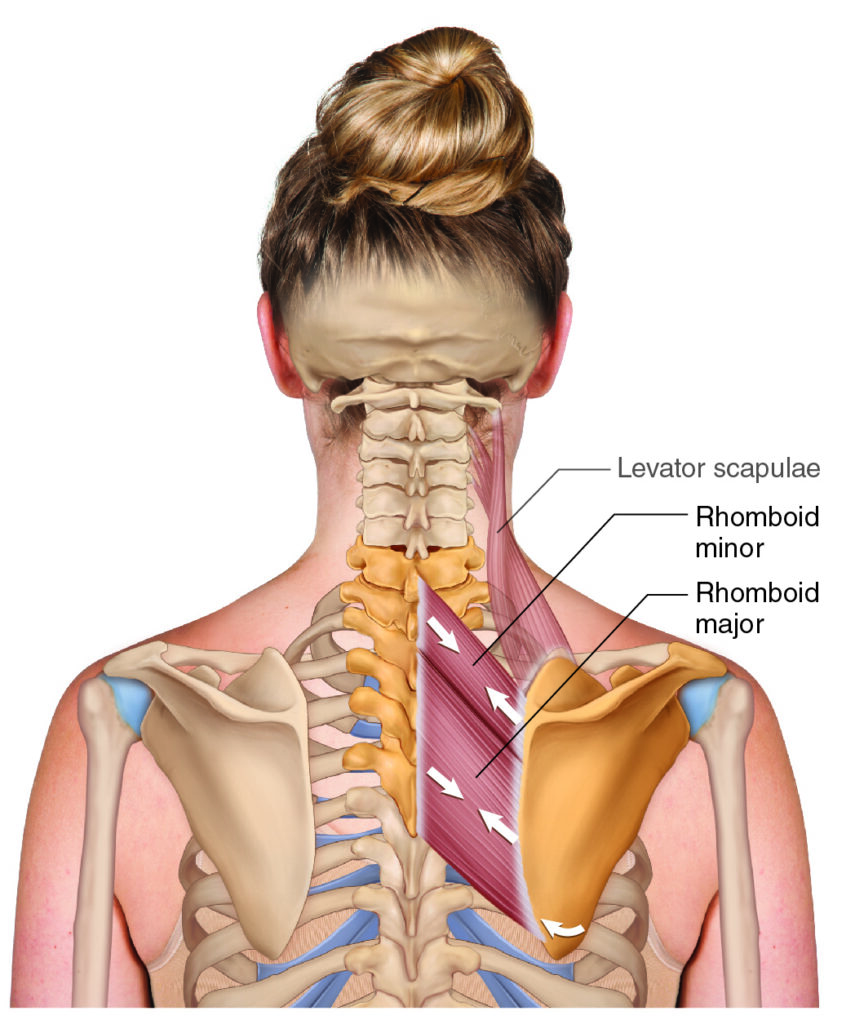
Rhomboids minor and major (permission: Dr. Joe Muscolino)
Quick Answer: The rhomboids are two upper back muscles (rhomboid minor and major) located between the spine and scapula. They retract, elevate, and downwardly rotate the scapula, and play a critical role in upper crossed syndrome (UCS) — likely the most common postural distortion pattern in the human body.
Introduction
The rhomboids are especially important muscles to learn and know about, not only because, like any muscle, they can become painful and dysfunctional, but because they are complicit in the postural distortion pattern known as upper crossed syndrome.
The rhomboids are two muscles located in the upper thoracic (interscapular) region between the spine and scapula. They are the rhomboid minor and rhomboid major, with the rhomboid minor located immediately superior to the rhomboid major. They are so-named because of their characteristic shape being a rhombus, in other words, a four-sided parallelogram, meaning each two opposite sides are parallel with each other (in the case of the rhomboids, because the angles between the sides are not 90 degrees, the rhomboids are not rectangular). And the rhomboid minor, as its name implies, is smaller than the rhomboid major (which is larger than the rhomboid minor).
Christmas Tree Muscles (Permission Dr. Joe Muscolino)
Given that a muscle’s joint actions are determined by its line of pull, which in turn is determined by the direction of its fibers, it is helpful to know how the rhomboids run between the spine and scapula. There is a cute gimmick to know and remember this. The rhomboids can be called the Christmas Tree muscles. In this metaphor, the spine forms the trunk of the tree, and the rhomboids on each side form the branches. And this helps us to understand that as the fibers run medially from the scapula to the spine, they also run superiorly; so, they run superomedially. And this tells us that not only do they pull the scapula medially toward the spine (retraction), they also pull it superiorly (elevation).
Rhomboid Muscle Attachments
The rhomboids as a group run from the spinous processes (SPs) of the lower cervical and upper thoracic spine to the medial border of the scapula.
More specifically, the rhomboid minor attaches proximally (origin) to the SPs of C7 and T1 and distally (insertion) onto the medial border of the scapula, at the root of the spine of the scapula.
The rhomboid major attaches proximally (origin) to the SPs of T2–T5 and distally (insertion) onto the medial border of the scapula, below the root of the spine of the scapula down to the inferior angle.
Note: The rhomboid minor has two SP attachments (C7, T1), and the rhomboid major is double that at four (T2, T3, T4, T5).
For an atlas of high-resolution downloadable and usable (in your teaching) muscle illustrations, click here.
Nearby Anatomy
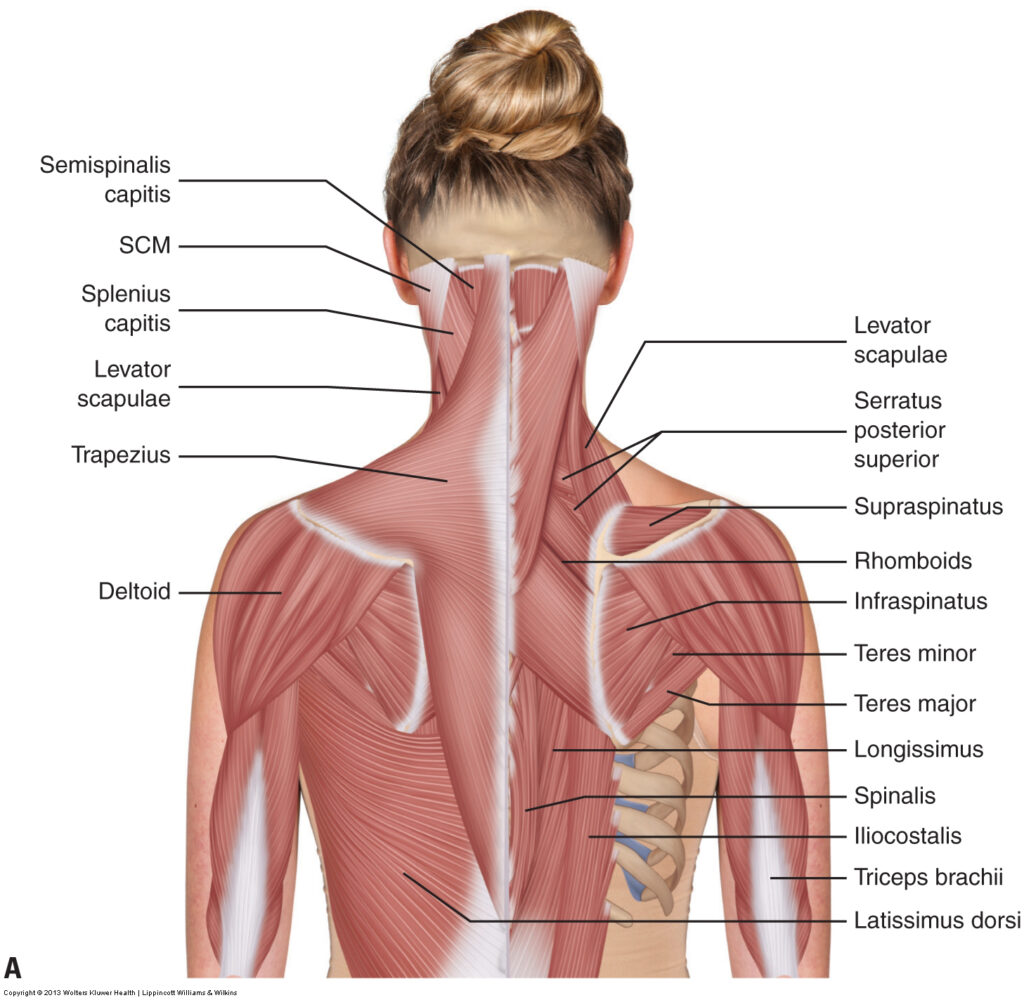
Posterior view of the musculature of the neck and upper back (permission: Dr. Joe Muscolino)
The rhomboids lie directly deep to the middle trapezius (middle trap). They are, themselves, superficial to the vertically-running paraspinal (erector spinae and transversospinalis) musculature. Also, deep to them would be the posterior ribcage.
All this is important, because if the client has pain and/or tightness (hypertonic, overly-facilitated, locked short/locked long, densification of tissues, either globally or focally as a myofascial trigger point/TrP) in this interscapular region, knowing the direction that the structures are running makes it quite easy to assess which structure is involved as the cause of the client’s pain and/or dysfunction. The paraspinals run vertically; the middle trap runs horizontally; the rhomboids run diagonally (superomedially from scapula to spine as stated), and the ribs angle slightly diagonally like the rhomboids, but more medially, somewhat like the middle trap; overall, the orientation of the ribs is between the angulation of the trap and rhomboids.
Rhomboid Joint Actions and Functions
The joint actions of a muscle can be figured out from its line of pull, which we know is superomedial from the scapula to the spine. Assuming that the spine is the fixed/stable attachment, then when the rhomboids concentrically contract and shorten, the scapula would be pulled toward the spine. How? Superiorly and medially (as stated above… remember Christmas Tree Muscles), hence, the rhomboids would elevate and retract the scapula (shoulder girdle) at the scapulocostal (ScC) joint (aka as the scapulothoracic/ScT joint). And both rhomboid minor and major could equally perform these joint actions, although the major would be stronger given it is larger.
But the rhomboids can also rotate the scapula. Looking at the how they would pull the lower medial border up toward the spine, they would pull the inferior angle of the scapula up and in (superiorly and medially) toward the spine; this motion is called downward rotation of the scapula (at the ScC joint). Considering the lever/moment arm, the lower fibers would be much better at this action, therefore, the rhomboid major is a stronger scapular downward rotator than is the minor.
But the rhomboids cannot do any of these isolated joint actions. Because they have one line of pull, they must create an oblique-plane motion that is a combination of these individual cardinal-plane component joint actions. In other words, the rhomboids must create a motion that is both retraction AND elevation (and the rhomboid major especially must also create downward rotation) of the scapula.
And this conversation so far is only considering the rhomboids acting in an open-chain scenario in which the spine is fixed/stable and the scapula is mobile (which is the more common scenario to be fair). But if the scapula were to be held stable (perhaps the hand is holding onto a stable immovable object so the upper extremity is fixed/stable), we have a closed-chain scenario, then the spine would have to move toward the scapula instead. Looking at the line of pull, we see that the SPs would rotate toward the scapula on that side (which would be called contralateral rotation because rotation is named for the orientation of the anterior aspect of the spine). So, chronic tightness in the rhomboids could result in joint dysfunction of the upper thoracic spine.
Rhomboids and Upper Crossed Syndrome
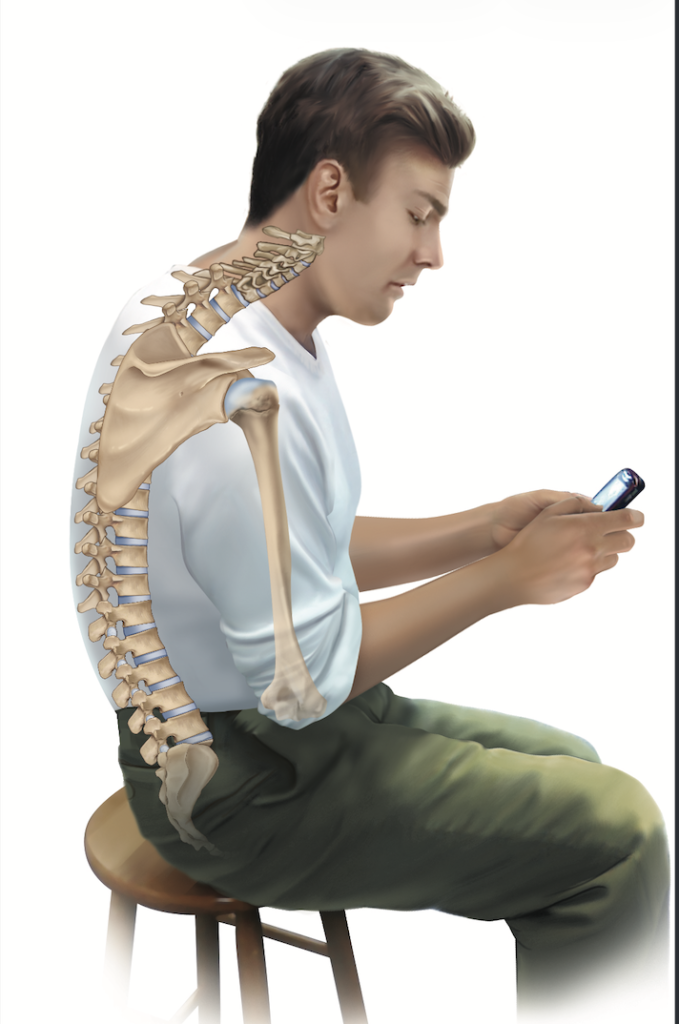
Upper Crossed Syndrome posture (Permission: Dr. Joe Muscolino)
Upper crossed syndrome (UCS) is a postural distortion pattern characterized by hyperkyphosis of the thoracic spine, hypolordosis of the lower cervical spine, with hyperlordosis (hyperextension) of the upper cervical spine (primarily atlanto-occipital joint) and …protraction of the shoulder girdles and medial rotation of the arms at the GH joints.
The relationship that the rhomboids have with UCS is that at baseline tone, the protractors of the shoulder girdle (e.g., pectoralis minor) are tighter than the retractors (rhomboids and the entire trapezius, primarily the middle trapezius). Using the pectoralis minor as the principal protractor, the pec minor is locked short, and the rhomboids are locked long. Both locked-long and locked-short muscles are tight (“locked”), and they are both weak (via the length tension relationship curve), so both protractors and retractors need to be loosened AND strengthened. But a greater emphasis needs to be placed on loosening the locked-short pec minor and strengthening the locked-long rhomboids.
A note regarding UCS: This is likely the most common postural distortion pattern found in the human body. It was always common for people to fall into the rounded shoulders of UCS, but with the advent of handheld digital devices (principally smart phones), the incidence of UCS syndrome is exploding. It is the responsibility of every manual/movement therapy practitioner to assess for UCS and appropriately treat, as well as counsel the client for what they can do for this condition.
Palpating the Rhomboids

Palpation position for the rhomboids (Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual)
Palpating the rhomboids (Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual)
To palpate the rhomboids, have the client prone on the table with their hand in the small of their back; placing the hand in the small of the back places the arm into adduction and extension at the GH joint. Then ask the client to lift their hand toward the ceiling, which requires active extension of the arm, which calls upon not only arm extensors to engage, but also retractors and downward rotators of the scapula at the ScC joint (via scapulohumeral rhythm). The rhomboids are both retractors and downward rotators, so they engage. Further, the upper trap, as well as some of the upper aspect of the middle trapezius are upward rotators of the scapula, so they are reciprocally inhibited and therefore relaxed, so it easier to palpate through them.
Do not place your hands in the interscapular area yet because they could block you from likely seeing the rhomboids engage and pop. Look especially for the inferior border to become visually prominent; if it is not visually apparent, it is likely easily palpable. Now, palpate the entirety of the rhomboids. Note that the upper attachment is on the SP of C7, which is the vertebral prominens; and then the superior border would be parallel with the lower border (remember opposite sides of a rhombus are parallel). Have the client alternately engage and relax the rhomboids (by lifting the hand, and then relaxing it down), and feel for the rhomboids to harden and soften.
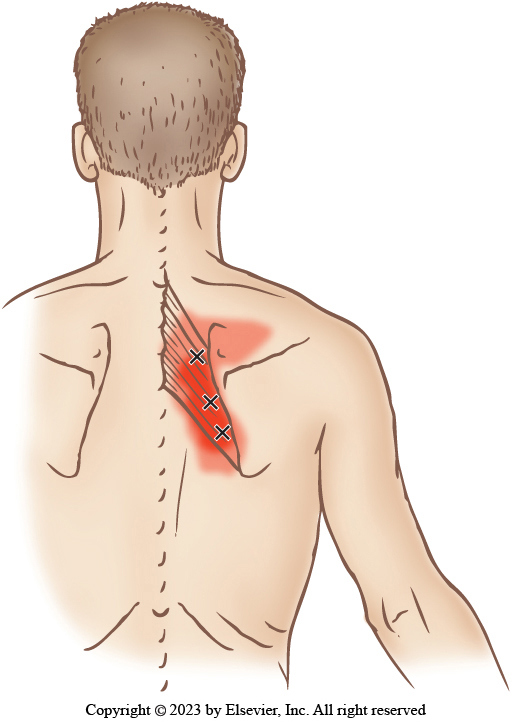
Rhomboids common TrPs and referral zones (permission: Dr. Joe Muscolino – The Muscle and Bone Palpation Manual)
Note: Because the rhomboids are so often locked long, they often develop myofascial trigger points (TrPs) in their effort to work against the locked-short pectoralis musculature.
Stretching the Rhomboids
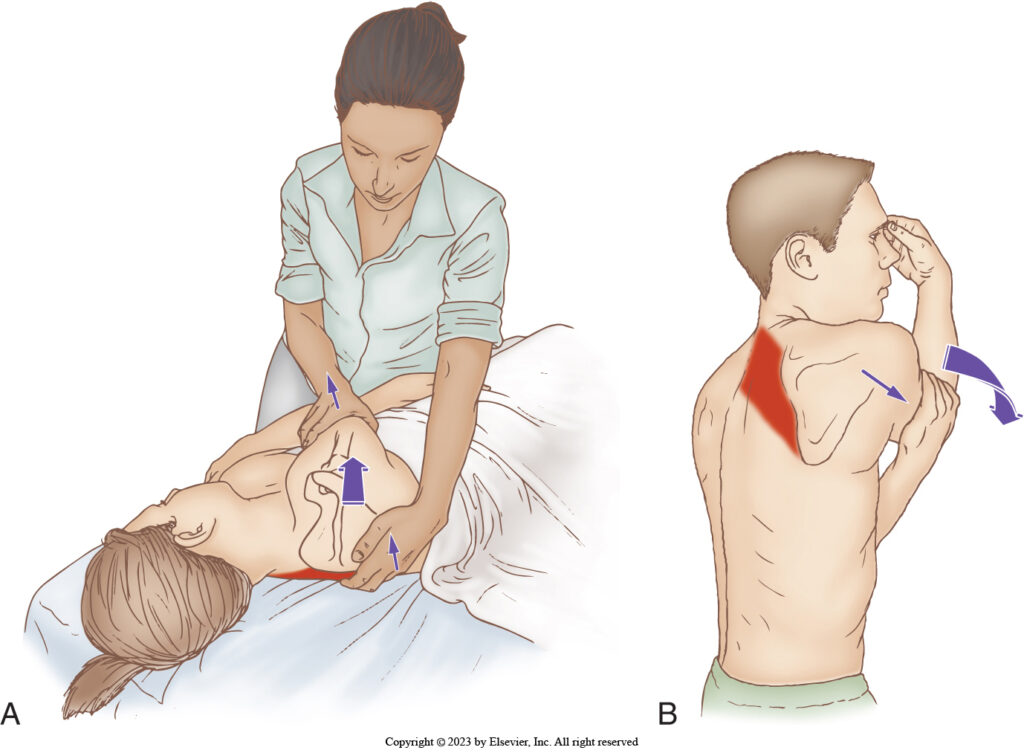
Stretching the rhomboids: therapist-assisted and client self-care (Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual)
Stretching is a process in which the target muscle is lengthened; a muscle’s joint action is the concentric shortening function of the muscle. Therefore, to stretch the target muscle, simply do the opposite of its joint action(s). The rhomboids retract and elevate the scapula, so they are stretched by protracting and depressing the scapula. This is facilitated by using the arm as a lever to move the scapula.
Massaging the Rhomboids
Certainly, if TrPs and/or any tightness of the rhomboids are found upon palpation assessment, the rhomboids can be massaged. But given how often they are functionally weak as part of UCS, they often need to be strengthened. This can be done many ways. It can simply be movement of the scapula into retraction and elevation, via movement of the arm into extension and abduction. Free weights can be used and/or movement can be against resistance with elastic tubing or bands; or via machines in the gym. Even playing sports such as tennis, pickleball, or padel will work the rhomboids during the backswing.
Frequently Asked Questions About the Rhomboid Muscles
What do the rhomboid muscles do? The rhomboids retract, elevate, and downwardly rotate the scapula. The rhomboid major is the stronger downward rotator due to its longer lever arm for rotation.
Where are the rhomboids located? The rhomboids are located in the upper thoracic (interscapular) region, between the spine and the medial border of the scapula, directly deep to the trapezius.
What is the difference between rhomboid minor and rhomboid major? The rhomboid minor attaches to the spinous processes of C7 and T1 and is smaller. The rhomboid major attaches to T2–T5, and is larger and stronger. Because the major attaches lower on the medial border of the scapula, it is a more effective downward rotator of the scapula.
How are the rhomboids related to upper crossed syndrome? In upper crossed syndrome, the rhomboids are typically locked long and functionally weak due to the overactivity of the opposing pectoralis minor. Treatment emphasizes stretching the pec minor and strengthening the rhomboids.
How do you stretch the rhomboid muscles? Because the rhomboids retract and elevate the scapula, they are stretched by doing the opposite: protracting and depressing the scapula, using the arm as a lever.
How do you strengthen the rhomboids? The rhomboids can be strengthened through scapular retraction exercises using free weights, resistance bands, cable machines, or sport activities like tennis, pickleball, and padel.
Conclusion
Every muscle can be tight and/or contain myofascial TrPs that necessitate treatment. Any muscle can be functionally weak and need strengthening. But the rhomboids are unusually important to be assessed and appropriately treated because of their involvement in what is likely the most common postural distortion pattern in the human body, upper crossed syndrome (UCS). They often need to be strengthened, but they also often develop TrPs and need massage to alleviate them.

Dr. Joe Muscolino
Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com,
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
