Self-care for the client/patient:

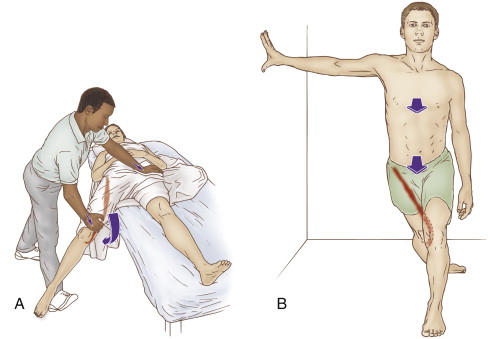
Therapist-assisted and self-care stretch for the sartorius. Permission: Joseph E. Muscolino. The Muscle and Bone Palpation Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. (2016) Elsevier.
Self-care for meralgia paresthetica involves removing the physical stress factors that could contribute to the condition: avoidance of clothing or belts that are tight and/or press against the anterior hip, losing excess weight, and avoiding offending postures and activities. Icing can be recommended to reduce pain. If tightness of hip flexor musculature is present, application or moist heat followed by hip flexor lunge stretches should be recommended. The lunge stretch can be focused on the tensor fasciae latae (TFL) by adding lateral (external) rotation to the thigh in back because the TFL is a medial (internal) rotator; similarly, adding medial rotation to the thigh in back focuses the stretch on the sartorius because it is a lateral rotator. Curl-ups/crunches can be recommended to strengthen the anterior abdominal wall.
Medical approach:
The medical approach is to counsel the patient to remove physical stressors that might contribute to the condition. Additionally, non-steroidal anti-inflammatory (NSAID) or over the counter pain killer (analgesic) medication is often prescribed. If the condition is more severe, steroidal anti-inflammatory (cortisone/prednisone) or narcotic analgesic medication might be prescribed. Nerve block injections are also possible.
Manual therapy case study:
Jacque is a 45-year-old carpenter who has been experiencing tingling and pain in the outside of his right thigh for the past month. Jacque weighs 185 pounds and is 6 feet tall. He does not recall any trauma or precipitating event that would have caused the symptoms. He notices that the lateral thigh symptoms seem to be worse on workdays than during the weekend. His symptoms worsened over the past week so he consulted his massage therapist who does clinical orthopedic work.
The therapist performed passive straight leg raise (SLR), slump test, cough test and Valsalva maneuver, all of which were negative. His low back and hip joint ranges of motion are within normal limits, except for decreased hip joint flexion and extension. Palpation of lumbar extensor and gluteal musculature revealed mild tightness bilaterally, but no myofascial trigger point referral pain was elicited. His hamstrings were moderately/markedly tight bilaterally. His right-sided anterior hip flexor musculature was moderately tight and tender to palpation, with pressure applied to the sartorius slightly increasing the tingling into Jacque’s lateral thigh. Postural examination revealed that Jacque stands with his knee joints hyperextended, his femoral heads projected anteriorly, and his pelvis in excessive posterior tilt with his low back rounded. Examination of his lateral thigh reveals no local injury or irritation. Pinwheel sensory examination confirms that his paresthesia is confined to the distribution pattern of the lateral femoral cutaneous nerve. During verbal history, the therapist asked Jacque about his tool belt and Jacque confirmed that it is very heavy because of all the tools that are attached and hanging from it.
Given that Jacque has been experiencing paresthesia (altered sensation) into his lateral thigh, meralgia paresthetica is the likely assessment. To confirm this, the therapist looked to both rule out other possible conditions that could cause his symptoms and look for any of the usual physical stressors that might cause meralgia paresthetica. In Jacque’s case, there is no indication of the presence of any other condition. And Jacque’s use of a heavy tool belt, his standing posterior pelvic tilt posture, and the tight sartorius referral into the lateral thigh confirm the likelihood of meralgia paresthetica.
Because the major thrust of treatment for meralgia paresthetica is modifying behavior, the therapist began the session by discussing with Jacque the importance of not wearing the tool belt until his symptoms were under control; and then lightening the weight of the tool belt to prevent the condition from returning into the future. The therapist also explained how Jacque’s posture might be contributing to his condition, recommending that Jacque pay attention to not hyperextend his knees when standing, and that he try to avoid rounding his back when sitting and standing. Because tight hamstrings could exacerbate this posture, the therapist recommended that Jacque use moist heat followed by hamstring stretching. A standing lunge stretch for the hip flexors was recommended. To increase its focus on the sartorius, the therapist instructed Jacque to medially rotate the thigh at the hip joint (by turning his foot inward) for the limb in back.
The focus of the therapist’s hands-on work was to relieve the tightness in Jacque’s hamstrings and hip flexors, with particular attention paid to the sartorius. This was done by using moist heat, followed by soft tissue manipulation (massage) and stretching. The therapist began with Jacque supine. A moist heat pack was placed on the anterior hip for five minutes. The hip flexors were then worked with cross-fiber and longitudinal strokes for five to ten minutes. Jacque was then placed side-lying on his left side and the sartorius was further worked, along with the gluteal medius and minimus. Heat was applied for a few minutes to the lateral pelvis and thigh, and then the sartorius was stretched in both side-lying and supine positions. Jacque was then placed prone and heat, soft tissue manipulation, and stretching were done for his hamstrings bilaterally; contract relax (CR) (also known as PIR or PNF) and agonist contract (AC) stretching techniques were performed for the hamstrings. Any remaining time was spent on Jacque’s low back. This approach was repeated twice per week for four weeks.
At the end of four weeks, Jacques lateral thigh tingling and pain had entirely disappeared. Given the physicality of Jacque’s job, the therapist recommended proactive maintenance care for Jacque.
