Introduction to patellofemoral syndrome:
As its name states, patellofemoral syndrome (PFS) is a condition of the patellofemoral joint, which is located between the underside (posterior surface) of the patella and the articular surface of the distal femur (the intercondylar groove). Essentially, patellofemoral syndrome is osteoarthritis of the patellofemoral joint. In other words, it is a degenerative condition that involves breakdown of the articular cartilage in the early stages, and the development of calcium deposits/bone spurs in the later stages. If the condition progresses to the point that pain is felt, it is often termed patellofemoral pain syndrome (PFPS). Another term used to describe patellofemoral syndrome is chondromalacia patella, which is descriptive of the degenerative changes to the cartilage of the patella: chondro means cartilage; malacia means bad/unhealthy. The term chondromalacia patella was once more popular, but is increasingly being replaced with patellofemoral syndrome.
Causes:

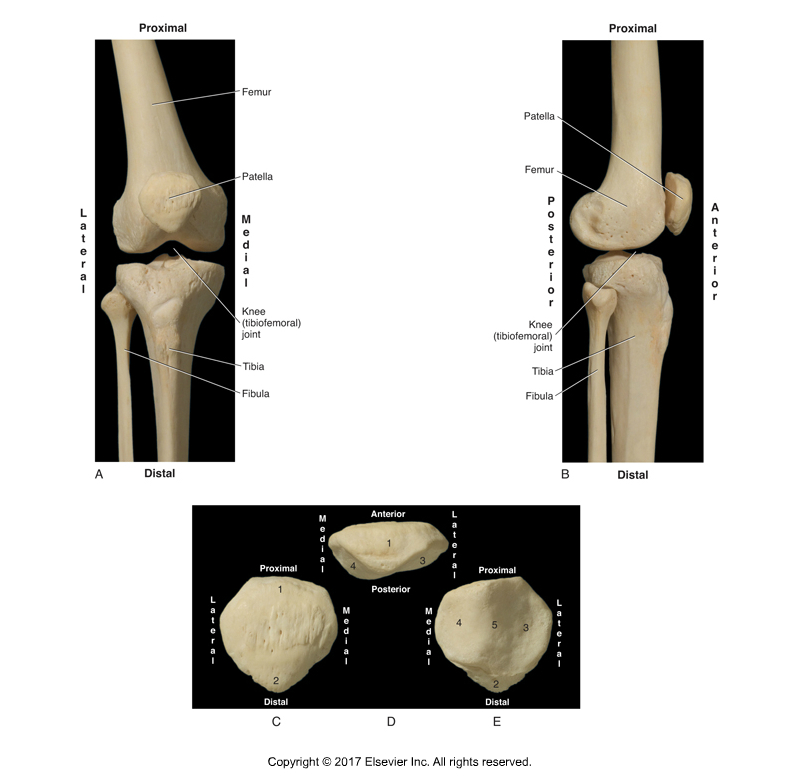
The patellofemoral joint is located between the patella and the femur. Permission: Joseph E. Muscolino. Kinesiology: The Skeletal System and Muscle Function, 3ed (2017), Elsevier.
Patellofemoral syndrome is osteoarthritis of the patellofemoral joint, therefore its root cause is essentially the same as osteoarthritis elsewhere in the body; that is, excessive physical stress placed through the joint. Therefore, anything that increases physical stress to the joint will be a potential cause of patellofemoral syndrome. Given that the accumulation of physical stress through the joints of the body is the natural consequence of aging, the degenerative changes of patellofemoral syndrome tends to increase as we get older.
Articular cartilage that lines joint surfaces is meant to absorb shock and other compressive forces that are transmitted through the joint. It is an indication of how much stress the patellofemoral joint encounters that the articular cartilage on the underside of the patella is the thickest articular cartilage in the human body.
The patella is a sesamoid bone that formed within the distal tendon of the quadriceps femoris musculature; its purpose is the hold the quadriceps musculature farther from the mediolateral axis of motion of the knee joint, increasing its leverage force and therefore its effective strength of extension at the knee joint. When the quadriceps femoris contracts, it pulls the tibia into extension at the knee (tibiofemoral) joint (in open-chain motion); it also tracks the patella upward (proximally), along and parallel to the femur, within the intercondylar groove (between the condyles) of the femur. During knee joint flexion, the patella tracks back downward (distally). However, not all of the pull of the quadriceps creates tibial extension and tracks the patella upward along the femur. A percentage of its contractile force pulls the patella posteriorly against the femur, placing a compressive and friction force upon the joint surfaces. Given how often we contract the quadriceps, it is clear why patellofemoral syndrome is such a common condition.
The quadriceps femoris is active with every step of the gait cycle. It is especially active during the stance phase to eccentrically brake knee joint flexion when the heel strikes the ground (so the knee joint doesn’t collapse Into flexion). The magnitude of this force increases if the client/patient is walking on a hard surface such as concrete/asphalt, running instead of walking, going downhill or downstairs (which requires greater eccentric braking force), or is overweight or carrying a heavy weight.
Beyond normal use/overuse of the joint via quadriceps femoris contraction, there are other factors that increase the physical forces through the patellofemoral joint. Many of these factors adversely affect the tracking of the patella within the intercondylar groove of the femur. If the patella does not track/glide smoothly within the groove, it will be pulled to the side, physically banging against the condyle. Most commonly, deviation of patellar tracking is lateral, causing excess force of the patella against the lateral condyle of the femur.
One cause of dysfunction patellar tracking is asymmetrical strength of pull of the vastus medialis and vastus lateralis. Often, the vastus lateralis is functionally stronger than the vastus medialis, resulting in the patella being pulled laterally against the lateral condyle as it tracks up the femur during knee joint extension. Another cause of dysfunctional patellar tracking is genu valgus. Genu valgus is a lateral deviation postural distortion (abduction) of the leg at the knee joint. Because of the orientation of the tibia and femur with genu valgus, the patella tracks laterally as it moves up the femur, banging into the lateral condyle.
Given that genu valgus is a cause of patellofemoral syndrome, anything that contributes to genu valgus also contributes to patellofemoral syndrome. One cause of genu valgus is an imbalance within the frontal plane musculature at the hip joint. If the hip joint abductors are weak and/or the adductors are tight, the posture of the thigh at the hip joint deviates toward adduction, which then predisposes the leg to deviate laterally at the knee joint, therefore genu valgus, dysfunctional patellar tracking, and patellofemoral syndrome. Weak lateral rotators of the thigh at the hip joint and/or tight medial rotators can also contribute. As the thigh falls into medial rotation, it also tends to adduct, predisposing the client/patient toward genu valgus and patellofemoral syndrome. Overpronation of the foot can also contribute to patellofemoral syndrome because overpronation results in excessive medial rotation of the entire lower extremity, which can affect tracking of the patella.
Even if there is not an imbalance between the lateral and medial aspects of the quadriceps musculature, if the overall baseline tone of the quadriceps is tight, the increased pull upon the patella can lead to wear and tear upon the joint and therefore patellofemoral syndrome. Ironically, even weak quadriceps femoris musculature can be a precipitating factor for patellofemoral syndrome. Proper joint function depends on stability as well as mobility; and strong quadriceps musculature increases the stability of the knee joint complex, including the patellofemoral joint, allowing for proper control and movement of the patella as it tracks along the femur.
Hyperextension (genu recurvatum) of the knee joint is another cause of patellofemoral syndrome because the posture of hyperextension jams the patella posteriorly against the femur. Overt trauma, such as a fall on the knee joint or an impact during a sporting competition, is another precipitating factor for patellofemoral syndrome due to the direct physical forces placed through the joint surfaces. Even the presence of patellofemoral syndrome itself can cause further progression of the condition. Due to the cartilage degeneration, the joint surfaces are roughened. Therefore use of the joint causes friction of these rough surfaces against one another, further irritating and inflaming the cartilage, accelerating the progression of the condition.
