Forward head posture is extremely common, especially as we age. It is part of a larger posture dysfunctional pattern known as upper crossed syndrome.
To understand the pathomechanics behind an abnormal cervical curve, it helps to first understand the normal cervical spine. A normal healthy cervical spine should have a lordotic curve, also known as a lordosis. A lordotic curve is a curve of extension in which the upper cervical vertebrae extend back in the sagittal plane relative to the lower cervical vertebrae. The result is a curve that is concave posteriorly and convex anteriorly. The cervical lordosis is a secondary curve of the spine that forms after birth when the child lifts his or her head into extension to see his or her surroundings. When the normal cervical lordosis is decreased or lost entirely, it is termed a hypolordosis or hypolordotic cervical spine, commonly known as military neck. A decreased cervical spinal curve then results in the posture of the head being protracted or held forward (Fig. 21). In some cases, a client may even have a reverse cervical curve, in other words, a kyphotic cervical curve.
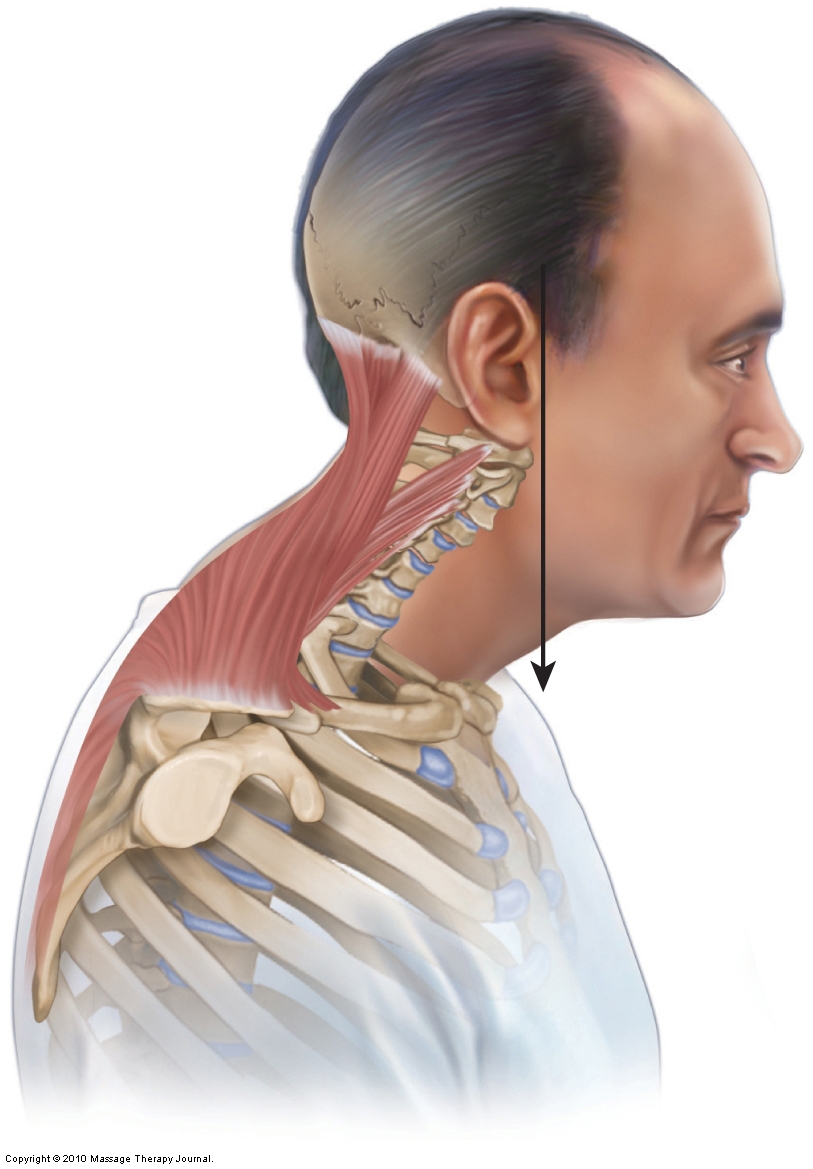
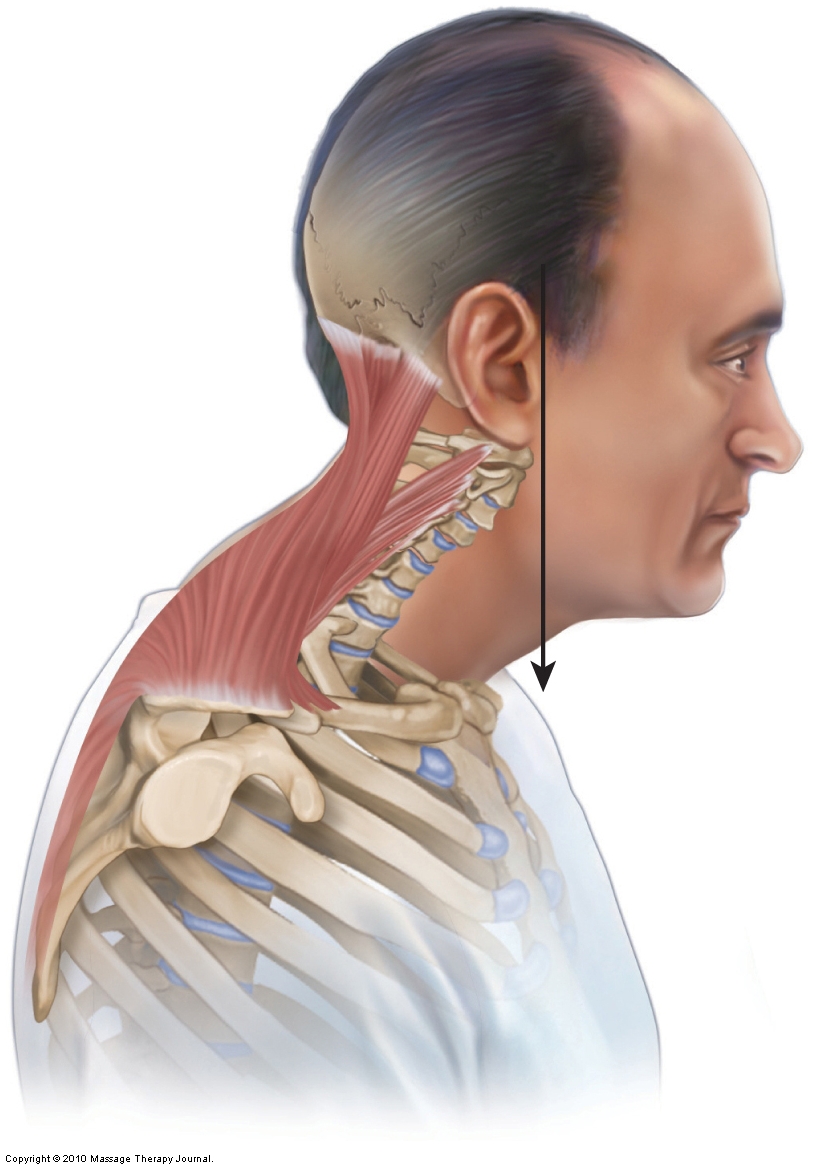
Figure 21. Forward head posture. Note that the center of weight of the head is anterior to the trunk.
Note: The Terms Lordosis and Lordotic
Many people use the terms lordosis and lordotic to denote an excessive and unhealthy lordotic curve/lordosis. It is important to understand whether the person is referring to a normal lordosis or an excessive lordosis in such cases. An excessive lordosis is most accurately termed a hyperlordosis/hyperlordotic curve.
Mechanism of Hypolordotic Cervical Curve and Forward Head Posture
The major benefit of the cervical spine’s lordosis is that it brings the position of the head back posteriorly to be balanced over the trunk (the weight centered directly over the trunk). This balances the weight of the head so that little or no effort is expended by the muscles of the neck and head to hold it in this position.
However, when the cervical curve is lost, the head is positioned anteriorly (protracted) such that its weight is no longer centered over the trunk (see Fig. 21). This anterior position of the head should cause the head and neck to fall in full flexion, resulting in the chin hitting the chest. This does not occur because posterior extensor musculature of the neck and head (e.g., upper trapezius, levator scapulae, splenius capitis, splenius cervicis, semispinalis capitis) contract isometrically to hold the head and neck in this imbalanced position. This results in chronic tightness of the posterior cervical extensor musculature. Therefore, although a hypolordotic cervical spinal curve does not itself cause pain and dysfunction, it does place an increased burden on the posterior musculature of the neck. It is the tightness of this musculature that usually causes the client’s symptoms. It also results in an adaptive shortening of the flexors of the neck on the anterior side. The result is dueling locked short – locked long musculature on the opposing anterior and posterior sides of the neck.
Causes of Hypolordotic Cervical Curve and Forward Head Posture
A hypolordotic cervical curve is most commonly the result of chronically holding the head and neck in a prolonged posture of flexion. The cervical lordotic curve forms as a child repeatedly lifts its head into extension, and therefore repeated postures of flexion can either decrease its formation and/or reverse it after it has formed. Unfortunately, postures of flexion are common and begin early in childhood when a child plays with toys or colors with crayons on a pad of paper held on the lap. These flexion postures continue in school, with pens and pencils replacing the crayon and computers and other digital devices replacing the pens and pencils. Depending on the type of work that a client does, flexion postures may continue throughout life. Even sleeping postures, such as sleeping on the back with a pillow that is too thick, can push the cervical spine into flexion, contributing thousands of hours to this posture. No wonder so many clients manifest with a decreased cervical curve! A hypolordotic cervical curve may also occur as a result of whiplash and consequent muscle spasms after a car accident.
Because a hypolordotic cervical curve does not bring the head back into extension, it causes the neck and head to follow the curve of the upper back’s kyphotic curve (the terms kyphotic and kyphosis can also be used to denote a normal degree of spinal curvature or an excessive unhealthy degree of curvature). This causes the neck to be placed anteriorly and the head to face downward; the greater the thoracic kyphosis (often as part of the larger postural dysfunctional pattern known as upper crossed syndrome), the more pronounced this altered posture. To bring the eyes upright as well as level the head for inner ear balance, the upper cervical extensors (e.g., suboccipitals, upper trapezius, splenius capitis, and semispinalis capitis) tighten and contract, creating a hyperlordosis of the upper cervical spine to compensate for the hypolordosis of the lower cervical spine. The general rule is that the greater the thoracic kyphosis, the greater the lower cervical hypolordosis and upper cervical hyperlordosis.
For this reason, the thoracic spine is often a silent saboteur, causing many of the pain and dysfunction patterns in our clients’/patients’ necks. So it imperative to thoroughly and accurately assess the thoracic spine in all clients/patients who present with any musculoskeletal condition of the neck!
Treatment Considerations in Brief for Hypolordotic Cervical Curve and Forward Head Posture
Massage and stretching of the posterior neck musculature are extremely beneficial in helping to decrease muscular tightness and spasms associated with hypolordosis. If the cause of this posture is tight anterior neck musculature, then that region must be addressed as well. Moist heat before stretching is also valuable.
Of course, with any treatment to the neck, there are always precautions and contraindications to consider.
Note: To the degree that the forward head posture is due to hyperkyphosis of the thoracic spine (upper crossed syndrome), then this more fundamental postural dysfunctional pattern must be addressed before any lasting and meaningful relief from forward head posture can be attained.
Note: This blog post article is the eighth in a series of 10 posts on
Common Musculoskeletal* Conditions of the Neck
The 10 Blog Posts in this Series are:
- Fascial Adhesions (and an introduction to musculoskeletal conditions of the neck)
- Hypertonic (tight) musculature
- Joint dysfunction
- Sprains and strains
- Pathologic disc conditions
- Osteoarthritis (OA)
- Thoracic outlet syndrome (TOS)
- Forward head posture
- Tension headaches
- Greater occipital neuralgia
(*perhaps a better term is “neuro-myo-fascio-skeletal”)
