Sacroiliac Joint Dysfunction
Sacroiliac joint dysfunction (SIJ dysfunction) is a condition in which there is unhealthy movement at the SIJ (dys means bad). There are two types of dysfunctional movement at the SIJ (and indeed at every joint of the body): hypomobility, which is decreased/insufficient motion; and hypermobility, which is increased/excessive motion.
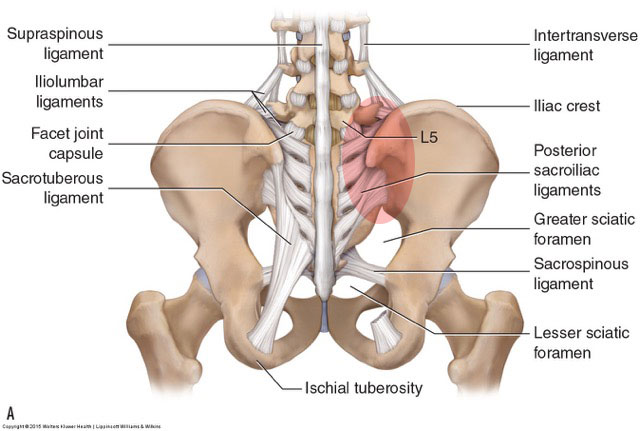
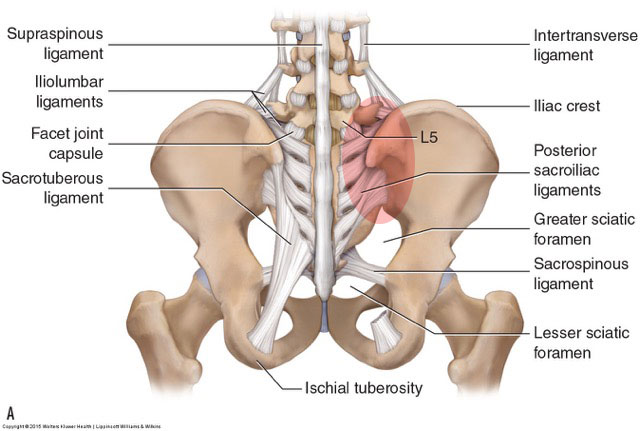
The sacroiliac joint is a common area for dysfunction. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
The sacroiliac joint (SIJ) is unique in that it is a transitional joint between the sacrum of the spine (axial body) and the ilium of the pelvic bone of the lower extremity. The SIJ is also unusual in that it begins as a synovial joint when we are young, and gradually transitions into a fibrous joint as we age. Even though motion at the sacroiliac joint is small, that motion can be very important because it functions as part of the axial spine and lower extremity. For this reason, and because SIJ dysfunction is so prevalent, this condition merits its own article.
It should be noted that SIJ motion is very controversial. Many physicians deny that the joint has appreciable movement that can be of any importance. However, looking at the placement of the SIJs, we see that they (along with the symphysis pubis joint) allow motion to occur between the two pelvic bones. This is important because of femoropelvic coupled motion patterns in which movement of the femur on one side of the body couples with movement of the pelvic bone on that side of the body. For example, when a soccer player kicks the ball with their right foot, the right femur flexes and couples with posterior tilt of the right pelvic bone, but the left femur and pelvic bone need to remain fairly stable in their position. This can only happen if there are functional joints between the right and left sides of the pelvis. Without SIJ motion, the entire pelvis would have to move as a fixed unit.
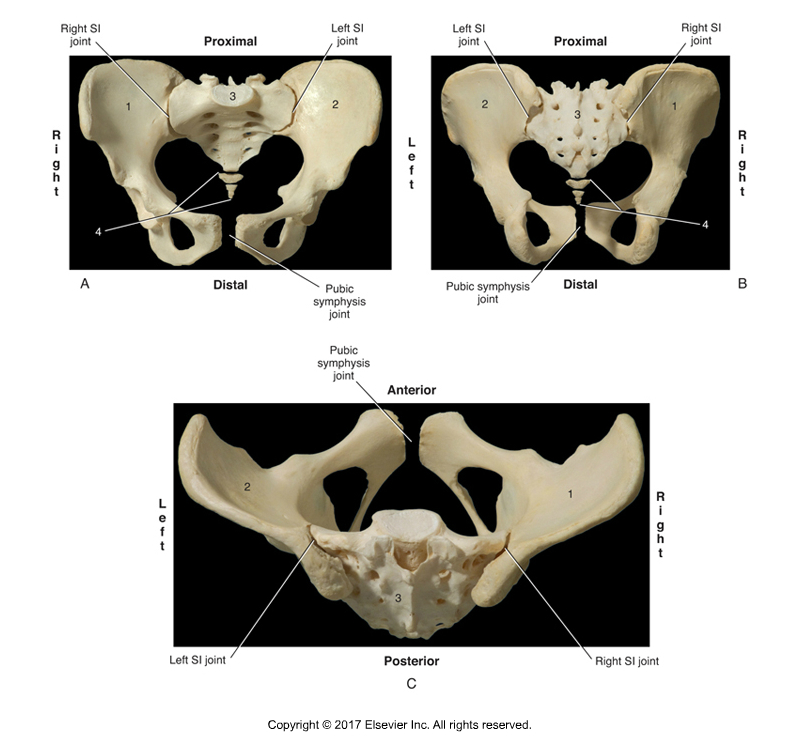
Sacroiliac Joint. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function 3ed (Elsevier) 2017.
Causes of Sacroiliac Joint Dysfunction
A hypomobile sacroiliac joint dysfunction occurs from either increased soft tissue tension (increased baseline muscle contraction tone and/or fascial adhesions that have accumulated in the soft tissues) that does not allow for the soft tissue stretching that occurs with movement, and/or bony obstruction (due to degenerative osteoarthritic bone spurs) that does not allow for the movement of the bones of the joint toward each other. A hypermobile joint occurs due to decreased soft tissue tension (laxity) that does not sufficiently limit the motion at the joint.
The SIJ is a heavily ligamentous joint with relatively few muscles that actually cross the joint itself. Therefore, hypomobility due to soft tissue tension as well as hypermobility due to soft tissue laxity is often fascial (ligamentous) in origin. Even if no injurious traumas occur to the SIJ, the compression and movement forces through the joint probably contribute to gradual deposition of fibrous tissue within the joint that is responsible for its transition from synovial to fibrous joint classification as we age. For this reason, middle-aged and elderly clients may be extremely locked and hypomobile due to the accumulation of microstresses of life, coupled with the sedentary lifestyle of modern society. Hypermobility is often due to sprain injuries of the SIJ, but may be due to repeated activities that involve stretching of the region (such as dance, gymnastics, or yoga).
Musculature can also factor in. There are deep upper fibers of the gluteus maximus that attach from the sacrum to the ilium. The piriformis also crosses the SIJ, running from the anterior sacrum over to the greater trochanter of the femur (but by also crossing the hip joint, will be somewhat compromised in its ability to properly stabilize the SIJ). The coccygeus also cross the SIJ. It attaches to the sacrum and coccyx and has its other attachments onto the ischium of the pelvic bone. Even the levator ani has fibers that effectively cross the SIJ because some of its fibers attach from the coccyx to the pelvic bone. And paraspinal muscles and the latissimus dorsi attach into the sacrum and ilium from above. These muscles may either increase their tone to limit motion at a hypermobile SIJ, or they may tighten due to SIJ pain or dysfunction and end up causing SIJ hypomobility.
The aforementioned causes of sacroiliac joint dysfunction are primary in nature in that they directly affect the structural integrity of one of the SIJs. However, SIJ dysfunction is often secondary in nature, compensating for dysfunction at the contralateral (other-side) SIJ. Dysfunctional motion at one SIJ often results in dysfunctional motion at the other SIJ. For example, if one SIJ becomes hypomobile, then the other SIJ may become hypermobile to compensate for the lost motion. Similarly, if one SIJ is hypermobile, then the other SIJ is not called upon to move as much and may become hypomobile in time.
