Self-care for the client/patient
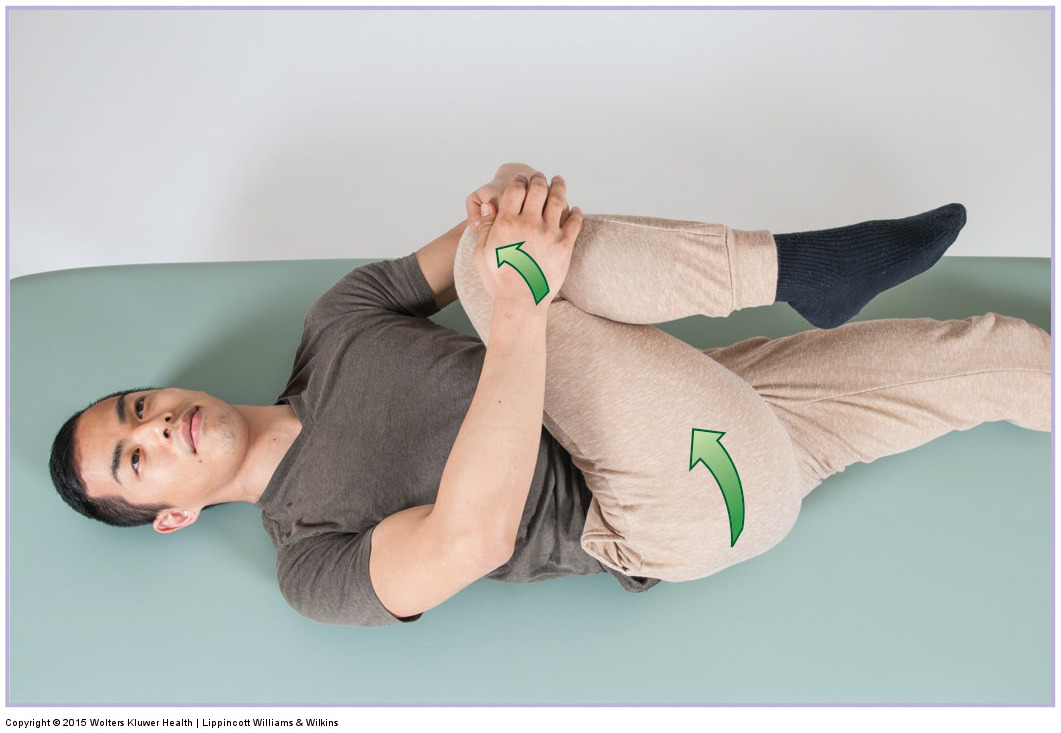
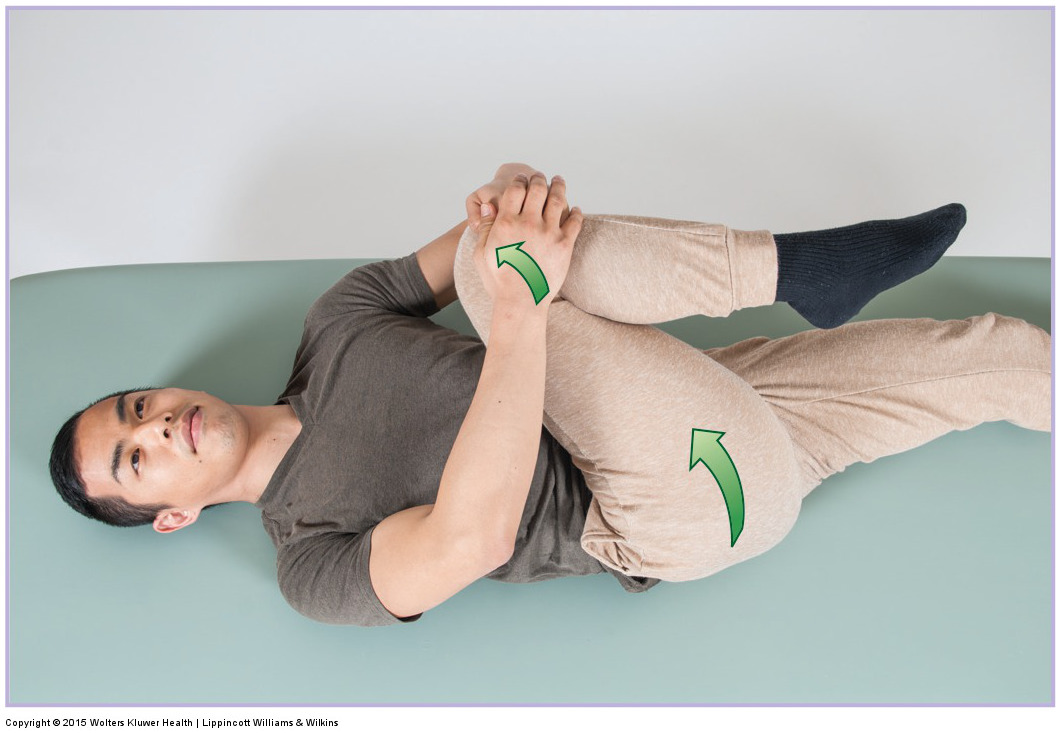
A self-care stretch for the sacroiliac joint. Permission: Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Recommend moist heat and stretching for a hypomobile sacroiliac joint (SIJ) and/or tight musculature that might be accompanying a hypomobile or hypermobile SIJ. Double knee to chest stretch and either the horizontal adduction or Figure-4 stretch for the piriformis should be recommended. Client/patient posture is often involved, so advice for proper posture should be given. Foremost amongst these is to avoid prolonged sitting and also prolonged standing. Bending, lifting, and twisting should also be avoided. If a SIJ is hypermobile, strengthening the associated musculature is extremely important.
Medical approach
It is rare that the medical community recognizes SIJ dysfunction as a condition. When they do, physical therapy is usually recommended. If the client/patient has an acute hypermobility due to a recent injury, then a SIJ brace will likely be recommended.
Chiropractic (and many osteopathic) physicians address SIJ dysfunctional hypomobility with Grade V (fast thrust) joint manipulation. Grade V manipulation is identical to Grade IV, except that a fast thrust is introduced. If you assess a SIJ hypomobility and your client has a chiropractic physician, referral to the chiropractor could and should be done. You may certainly continue to see the client/patient and even perform SIJ Grade IV mobilization, but the referral is in the best interest of the client. If the client is not a chiropractic patient, then improvement of the SIJ hypomobility will depend solely on your treatment.
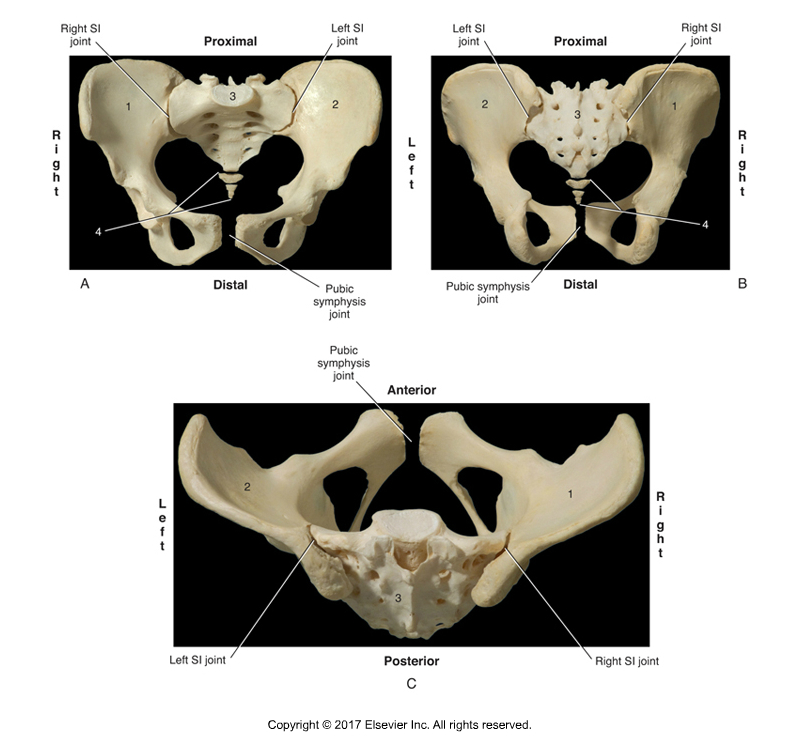
Sacroiliac Joint. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function 3ed (Elsevier) 2017.
Manual therapy case study
Giovanni is a 35-year-old medical illustrator who spends the vast majority of his time sitting at the computer. Over the past couple of weeks, he has been feeling mild dull pain in his left low back/hip area. Two weeks ago, the pain would begin after he had been sitting for longer than an hour. Now, sitting for 30 minutes or longer brings on the pain. He occasionally feels referral pain down into his posterolateral left thigh. When asked to indicate the location of his pain, Giovanni pointed directly to the area around his left PSIS.
During physical examination, Giovanni was negative to active and passive SLR tests, cough test and Valsalva maneuver, and Nachlas and Yeoman’s tests. Therefore, there was no indication of any space-occupying condition, or strain or sprain of the lumbar spine or sacroiliac joints. Static postural examination of the SIJ region showed that his right side of the sacral base is tilted and projecting further posterior than the left. Prone motion palpation (with pressure placed on the PSIS and sacrum) reveals that the right SIJ is clearly hypomobile. Motion palpation of the left SIJ shows that it is slightly hypermobile. Standing SIJ motion palpation confirms these findings. Giovanni’s piriformis and lumbosacral paraspinals are tight bilaterally. The upper medial fibers of the gluteus maximus are also tight on the left side. Also, pressure directly on the left PSIS and left side of the sacrum reproduces the pain pattern that Giovanni has been feeling.
Given the findings of the physical examination, the therapist determined that Giovanni’s right SIJ is hypomobile, causing his left SIJ to be slightly hypermobile as a compensation, and that the overuse of the left SIJ is causing pain. The therapist recommended two massages per week for three weeks.
Each session consisted of 10-15 minutes of medium pressure soft tissue manipulation to the prone client’s/patient’s entire spine and pelvis. While the upper back was being worked, a moist heating pad was placed on the client’s/patient’s SIJ region. The therapist then performed deeper pressure work into the musculature of the client’s/patient’s buttocks bilaterally, with particular emphasis on the right side. The client/patient was then stretched into single knee to chest (first right and then left) for the gluteals on each side, double knee to chest for the lumbosacral paraspinal musculature, and horizontal adduction stretch (first left and then right) for the piriformis. After this, the therapist performed joint mobilization for the client’s/patient’s right-side SIJ, directing pressure into the joint by contacting both the PSIS and sacrum, and orienting the line of pressure in various directions. With whatever time was left the therapist worked the client’s/patient’s lower extremities.
This approach was repeated at each successive session, with the intensity of all modalities increasing with each treatment as Giovanni’s right SIJ gradually loosened. At the end of three weeks, Giovanni’s right SIJ hypomobility was sufficiently resolved (approximately 75% motion restored) that his left SIJ was not being overused having to compensate for the right side. As a result, his right SIJ pain was gone. The therapist recommended that Giovanni be proactive and come in for maintenance care as often as possible. The therapist also recommended that at work Giovanni get up from sitting every hour and walk around and stretch for a few minutes. It was also recommended that Giovanni begin a strength training program.
