Frozen Shoulder
 Frozen shoulder, also called adhesive capsulitis, is a common shoulder condition characterized by loss of range of motion (ROM) in the shoulder (glenohumeral) joint. Pain and the feeling of stiffness often also occur. The average length of symptoms is 30 months. Spontaneous recovery sometimes occurs, but the condition may become chronic. It has been classically stated that the cause of frozen shoulder is chronic capsule inflammation and fibrotic adhesion of connective tissues surrounding the glenohumeral joint. However, the pathomechanics of this condition are not yet fully understood.
Frozen shoulder, also called adhesive capsulitis, is a common shoulder condition characterized by loss of range of motion (ROM) in the shoulder (glenohumeral) joint. Pain and the feeling of stiffness often also occur. The average length of symptoms is 30 months. Spontaneous recovery sometimes occurs, but the condition may become chronic. It has been classically stated that the cause of frozen shoulder is chronic capsule inflammation and fibrotic adhesion of connective tissues surrounding the glenohumeral joint. However, the pathomechanics of this condition are not yet fully understood.
Research Study
Researchers from Australia recently conducted a preliminary cross-sectional observation study to investigate the feasibility of a muscle guarding component to movement restriction in patients with idiopathic frozen shoulder.
Five patients with painful, global restriction of passive shoulder movement volunteered for this study. The patients were scheduled for capsular release surgery for frozen shoulder. Passive abduction and external (lateral) rotation ranges of motion (ROM) were measured before and after the administration of general anesthesia.
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s continuing education video streaming subscription service for manual therapists and movement professionals, has six folders with video lessons on Manual Therapy Treatment, including an entire folder on Stretching, as well as a folder on Pathomechanics, another on Anatomy, and many more? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
Results
The results showed that passive abduction ROM increased following anesthesia in all participants, with increases ranging from approximately 55°–110° of pre-anesthetic ROM. Three of these participants also demonstrated substantial increases in passive external rotation ROM following anesthesia ranging from approximately 15°–40° of pre-anesthetic ROM.
See the video here https://twitter.com/LuiseHollmann/status/1017339041803481088
Conclusion
This case series of five patients with frozen shoulder demonstrates that active muscle guarding may be a major contributing factor to movement restriction in some patients who exhibit the classical clinical features of idiopathic frozen shoulder. These findings highlight the need to reconsider our understanding of the pathomechanics of frozen shoulder.
Comment by Joseph E. Muscolino
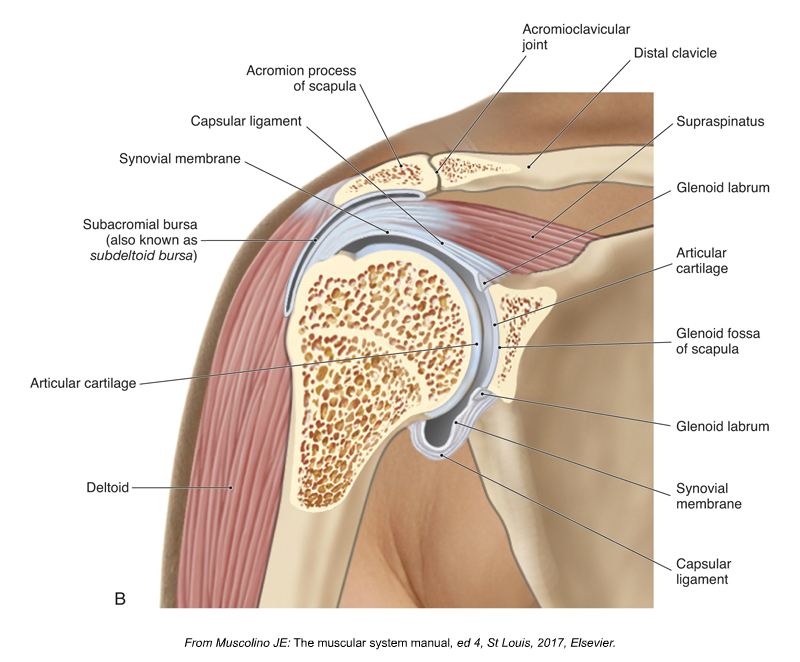
Frontal plane section through the right glenohumeral joint. Figure credit: Kinesiology – The Skeletal System and Muscle Function, 3rd Edition, 2017, Joseph E. Muscolino, Elsevier.
That muscle guarding / muscle tightness / muscle hypertonicity / overly facilitated musculature should be able to restrict joint range of motion, including in patients/clients with frozen shoulder should suddenly become a relevant finding is quite interesting to me. I learned 35 years ago that frozen shoulder would usually have two stages. Stage 1, called Neurogenic Frozen Shoulder, would be due to muscle hypertonicity (caused, as its name implies by the nervous system facilitating / tightening musculature). Then because the joint had not moved for some time, Stage 2 called Adhesive Capsulitis, would then be caused by the accumulation of fascial adhesions (as the “adhesive” implies). Muscle guarding for any joint that the nervous system perceives as fragile / vulnerable / injured is a well-recognized and well understood concept. Fascial adhesions occurring in any tissue that does not have movement is also a well-recognized and well understood concept (please see Gil Hedley’s Fuzz Speech video for a better appreciation of this). I am very happy that a new research study bears out these concepts, but slightly disappointed that it requires an evidence-based research study for us to apply fundamental principles of neuromyofascial tissue mechanics and pathomechanics to frozen shoulder.
(Click here for the blog post article: What are the Causes of Frozen Shoulder?)
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s continuing education video streaming subscription service for manual therapists and movement professionals, has six folders with video lessons on Manual Therapy Treatment, including an entire folder on Stretching, as well as a folder on Pathomechanics, another on Anatomy, and many more? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
