Introduction
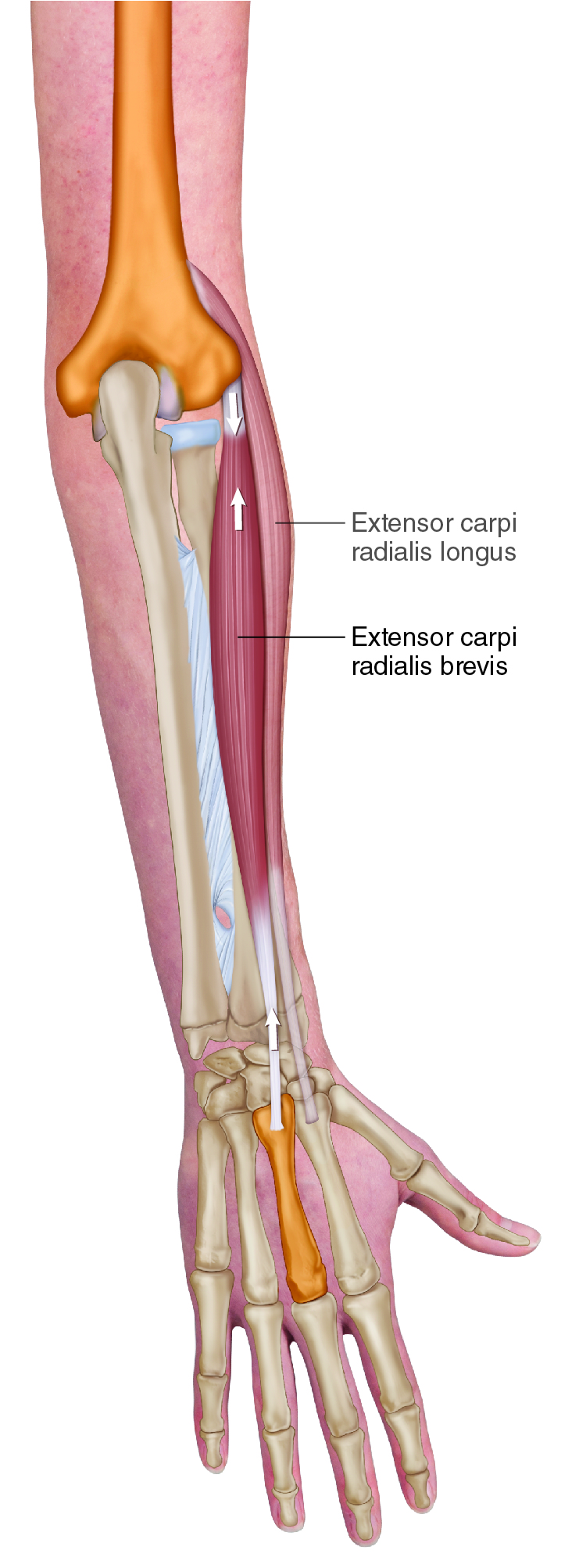
Extensor Carpi Radialis Brevis (ECRB). Permission Dr. Joe Muscolino (learnmuscles.com).
The extensor carpi radialis brevis (ECRB) is a member of the wrist extensor group. It is also one of the muscles of the common extensor belly/tendon; and of all the members of that group, it is the likely culprit when a person is experiencing tennis elbow.
Extensor Carpi Radialis Brevis Attachments
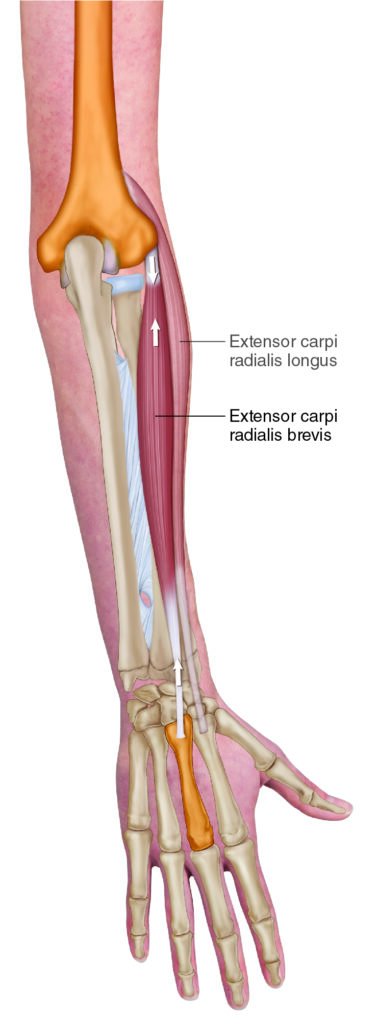
The extensor carpi radialis brevis (ECRB) attaches from the lateral humerus (origin) to the radial side of the hand (insertion).
More specifically, the ECRB attaches from the…
- lateral epicondyle of the humerus (via the common extensor belly/tendon)
to the
- posterior base of the 3rd metacarpal of the hand
Extensor Carpi Radialis Brevis Functions
The ECRB crosses the wrist joint posteriorly with a vertical direction to its line of pull, so it extends the hand at the wrist joint.
The ECRB crosses the wrist joint laterally (radially) with a vertical direction to its line of pull, so it laterally deviates (abducts) the hand at the wrist joint.
The ECRB also crosses the elbow joint, so it has function there as well. Even though it crosses the wrist joint posteriorly (extensor carpi literally means extensor of the wrist), as part of the radial group of muscles (along with brachioradialis and extensor carpi radialis longus), it actually crosses the elbow joint anteriorly, so it flexes the elbow joint (open-chain: it flexes the forearm at the elbow joint).
Nearby Anatomy
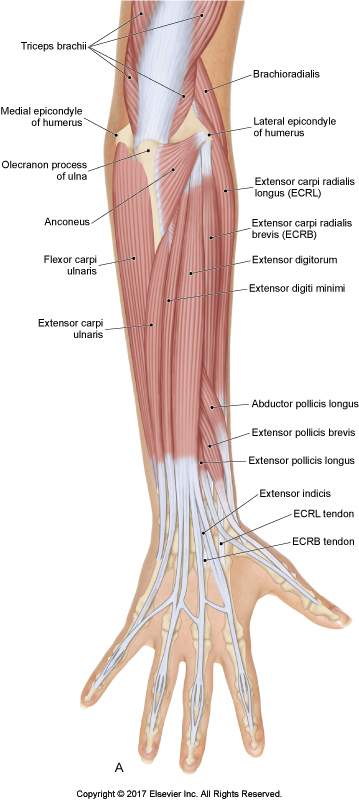
Posterior right forearm. Permission Dr. Joe Muscolino – The Muscular System Manual 5ed.
The ECRB is part of the radial group of muscles located on the radial side of the forearm; this group is composed of the brachioradialis, extensor carpi radialis longus (ECRL), and ECRB muscles.
It is also one of the muscles that create the common extensor belly/tendon (the structure involved in tennis elbow), composed of the ECRB, extensor digitorum, extensor digiti minimi, and the extensor carpi ulnaris (ECU).
And it is also one of the muscles of the wrist extensor group, along with the ECRL and the ECU.
Deep to the ECRB is the supinator muscle.
Involvement in Tennis Elbow
Tennis elbow is a condition of the common extensor tendon of the lateral forearm/elbow, which I believe should be expanded to be defined as the common extensor belly/tendon because the muscle bellies usually blend into each other before their tendons blend.
Tennis elbow involves use/overuse/misuse/abuse (to use the verbiage of the educator and author, Leon Chaitow) of the muscles of the common belly/tendon.
This condition usually begins with overuse tightness of the bellies of these muscles. This constant overuse pulling force is then transmitted into/through the common extensor tendon, resulting in tendinitis (itis means inflammation) of the common extensor tendon. And then the pulling force is transmitted into its bony attachment, resulting in a periostitis (inflammation) of the lateral epicondyle itself.
Tennis elbow is known by many names. Lateral epicondylitis describes the inflammation of the lateral epicondyle. This term is often used to describe this condition even if the periosteum of the lateral epicondyle has not yet become involved.
Given that when this condition becomes chronic, the inflammatory process usually dissipates, and what is left is degeneration of the fascia of the tendon, the term lateral epicondylitis is often replaced with lateral epicondylosis (osis is a more general term meaning condition of). However, even this term is perhaps not best because it continues to place the emphasis on the bone instead of the tendon, let alone the muscle bellies.
So, perhaps a better term to generally describe this condition would be lateral elbow tendinopathy, although even this term still ignores the muscle belly tissue itself.
The point that I am trying to make is that this condition usually begins first as a muscle tissue problem (overuse leading to muscle tightness and pain); then it progresses to being a tendon problem (tendinitis); and then can progress to being a bone problem (periostitis of the bony attachment of the tendon).
We can then layer on that the inflammatory itis stage often gives way to the fascial degeneration osis stage.
I doubt it would gain traction, but perhaps the best way to generally describe this condition with a term that would be inclusive of any and all stages would be lateral elbow myofascial syndrome. This would incorporate any muscle, tendon, or bone periosteal involvement.
Until the optimal term is coined, perhaps we can stick with tennis elbow, even though it is not a condition of the elbow joint, nor is it a condition that can only be caused by playing tennis.
What causes tennis elbow?
Most often, this condition is caused by overuse of the muscles of wrist and/or finger extension, resulting in excessive tension force pulling through the associated muscles and their tendons.
We usually think of concentric contraction of these muscles, meaning literally extending the wrist and/or fingers… for example, if the person has bad form during a tennis backhand and extends the hand at the wrist joint instead of keeping it neutral when striking the ball. However, the overuse of tennis elbow can also be caused by isometric contraction of the involved muscles. This can occur two ways.
Even if the person has perfect form when playing tennis and hitting a backhand, meaning that they keep their wrist neutral in position when striking the ball, it still requires (isometric) contraction of the wrist extensors because they have to oppose the force of the ball hitting the racquet which would otherwise cause the hand to collapse into flexion at the wrist joint.
And there is another major factor that can cause isometric overuse of the wrist extensor musculature. Whenever we are gripping an object, whether it is a tennis racquet, or a carton of milk, steering wheel, or pen for that matter, the muscles of finger flexion (primarily flexors digitorum superficialis and profundus) should also cause the hand to flex at the wrist joint. To prevent this, the wrist joint must be stabilized in the sagittal plane with a force of extension. This is provided by the wrist extensor musculature.
Now, of all the wrist extensors (ECRL, ECRB, extensor digitorum, extensor digiti minimi, ECU), why would the ECRB most likely be the culprit? Because if the extensor digitorum or the extensor digiti minimi were to contract, they would oppose the finger flexion, which is needed in the first case to grip the object.
So that leaves the ECRB, ECRL, and ECU. The problem is that whichever one of these muscles that is chosen as the sagittal-plane stabilizer would introduce a frontal-plane force into the wrist, which would then have to be countered by engagement of yet another muscle (which could be termed a second-order stabilizer).
The ECU would introduce ulnar deviation; and the two ECR muscles (B & L) would introduce radial deviation. But the ECRB is the closest to the midline so it would introduce the least frontal-plane force, so it would require the least contraction of second-order stabilizers.
So, the central nervous system will usually go to the ECRB to stabilize against the finger flexor contraction causing sagittal-plane wrist flexion. Hence, the ECRB is most often the muscle of the common extensor belly-tendon group that is involved with tennis elbow!
Note: Even though tennis elbow is named for the elbow, the elbow joint itself is not functionally involved. Functionally, tennis elbow is an overuse problem of the wrist and/or fingers.
Palpating the Extensor Carpi Radialis Brevis
The ECRB is the most posterior of the three muscles of the radial group in the lateral forearm. This group can be gently pinched away from the rest of the musculature of the forearm by using your thumb on one side, and your index and middle fingers on the other side.
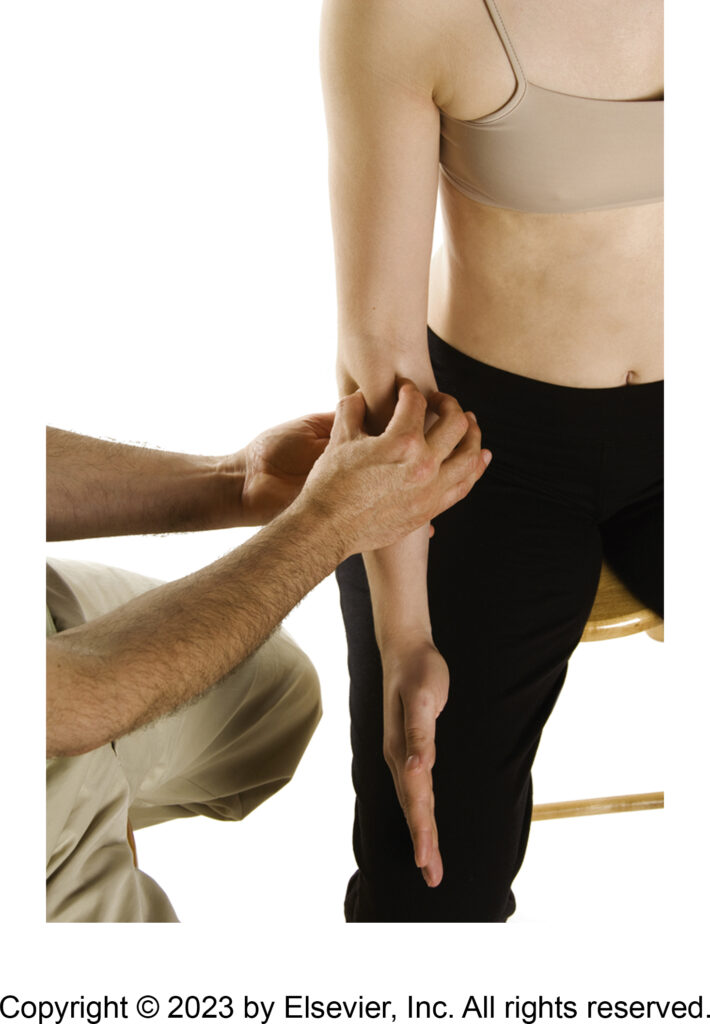
Pinching the radial group away from the body. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
Once the radial group has been pinched away, the ECRB will be the aspect of this musculature that is the most posterior, so it can be engaged with extension and/or radial deviation of the hand at the wrist joint (keep in mind that these motions will also engage the extensor carpi radialis longus).

Palpation of the ECRB. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
Once found, palpate this muscle to each of its attachments as well as you can.
The distal tendon of the ECRB can usually be easily found at the wrist by asking the client to make a fist (flexion of the fingers). Look for the tendon of the ECRB to pop and be visually apparent.
Stretching the Extensor Carpi Radialis Brevis
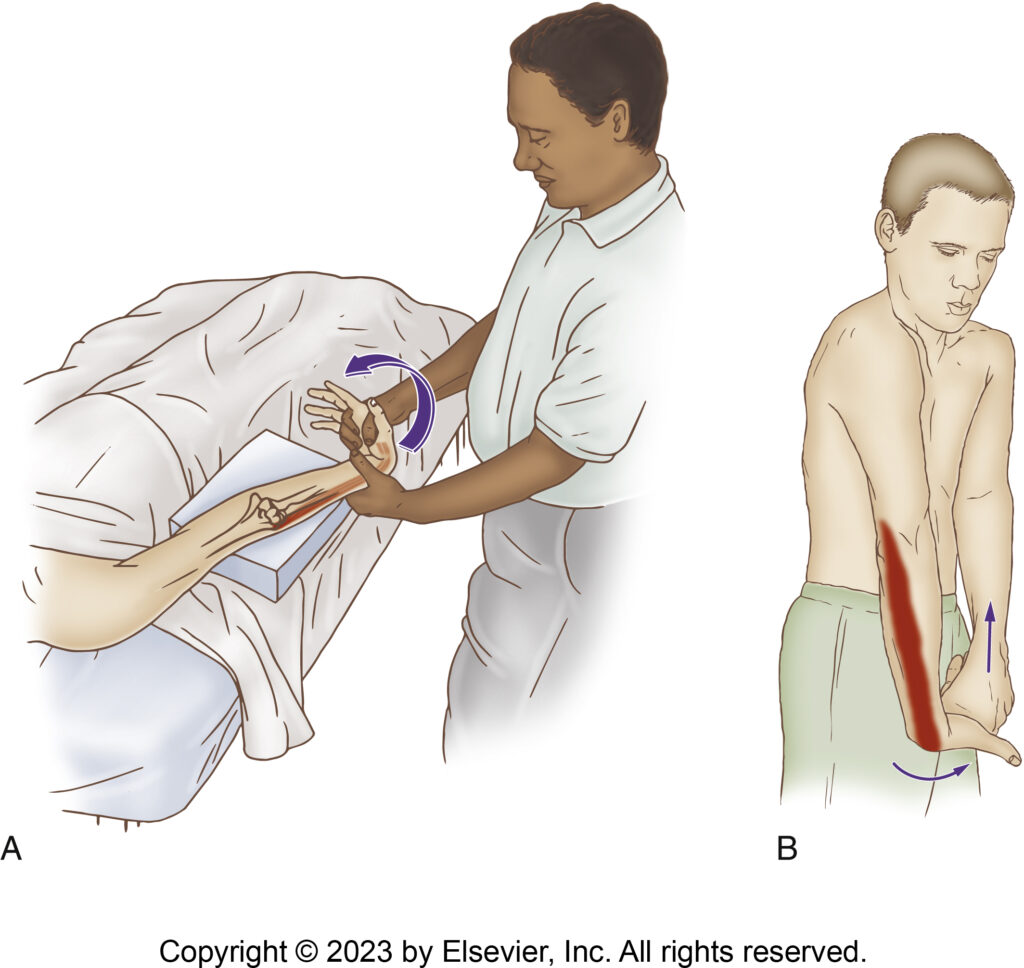
Stretching the ECRB. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The ECRB extends and radially deviates the hand at the wrist joint, so it can be stretched with flexion, along with some ulnar deviation of the hand at the wrist joint. Because this muscle crosses the elbow joint anteriorly, the elbow joint should be extended to increase the efficiency of the stretch.
Massaging the Extensor Carpi Radialis Brevis
Massaging the ECRB follows from the palpation protocol. Once the ECRB has been located and discerned from adjacent musculature (remember that it is challenging to discern the ECRB from the ECRL), it can be worked with any strokes that you like.
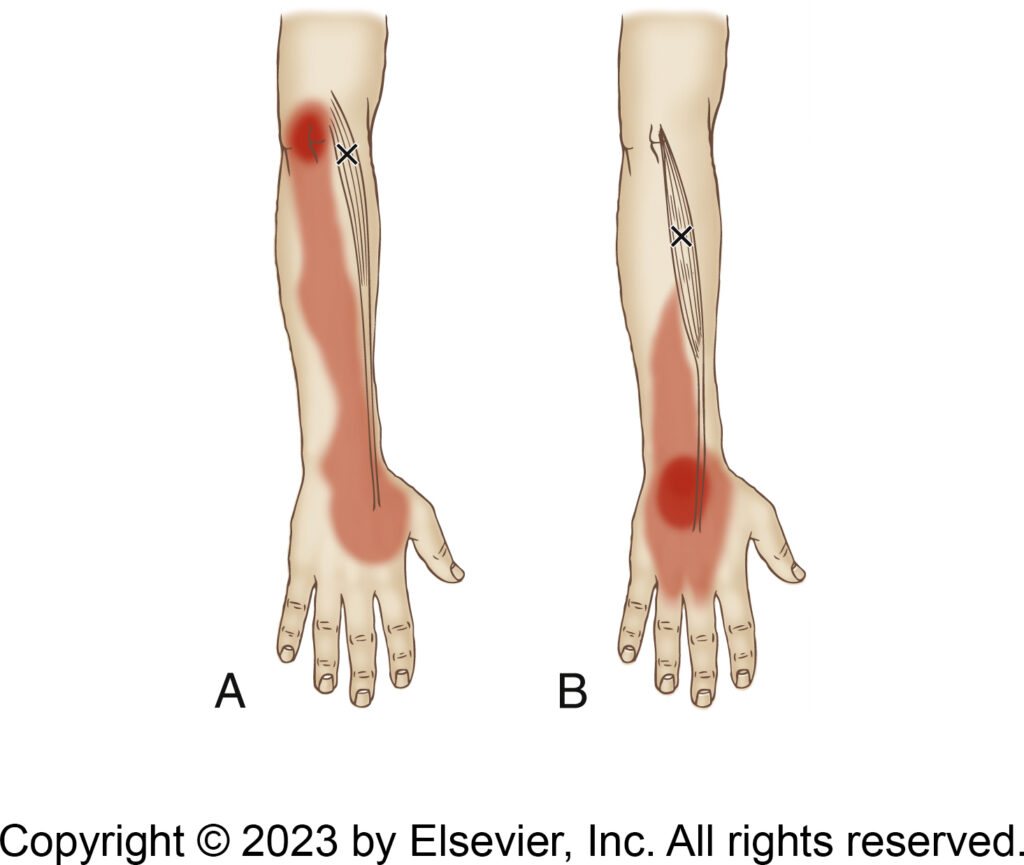
Trigger points in the ECRL (Fig A) and ECRB (
Fig B) and their referral zones. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
If longitudinal strokes are performed, generally it is the rule in the extremities to work from distal-to-proximal to go in the direction of venous drainage. However, with the muscles of the forearm, it is often logistically easier to work from proximal to distal. Cross fiber work is also extremely valuable to break of fascial adhesions, especially once the tendon has been reached.
Many therapists choose to do very deep work at the tendon when clients are experiencing tennis elbow. This is generally valuable when they are at the chronic osis stage, because it draws in new blood that can help to repair the degenerated fascial tissue.
Note: I would like to add that platelet rich plasma (PRP) injections can be very valuable for clients with tennis elbow who have fascial degeneration because the PRP helps the body to rebuild new fascial tissue. Although much more expensive than manual therapy, one PRP injection can likely replace 10 or more manual therapy sessions, so consider recommending to your clients to try PRP treatment.
Conclusion
As one of the muscles of the common wrist extensor belly/tendon group, the ECRB is often involved with tennis elbow, so the therapist should be conversant with its assessment and treatment.
Biography

Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com.
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
Frequently Asked Questions
What is the extensor carpi radialis brevis (ECRB)?
The extensor carpi radialis brevis (ECRB) is a member of the wrist extensor group and one of the muscles of the common extensor belly/tendon. Of all the members of that group, it is the likely culprit when a person is experiencing tennis elbow.
Where does the ECRB attach?
The ECRB attaches from the lateral epicondyle of the humerus (via the common extensor belly/tendon) to the posterior base of the 3rd metacarpal of the hand.
Why is the ECRB the most common muscle involved in tennis elbow?
The ECRB is closest to the midline among the wrist extensors, so it introduces the least frontal-plane force. The central nervous system will usually go to the ECRB to stabilize against the finger flexor contraction causing wrist flexion — hence, the ECRB is most often the muscle of the common elbow belly-tendon group that is involved with tennis elbow.
What is the difference between lateral epicondylitis and lateral epicondylosis?
Lateral epicondylitis describes the inflammation of the lateral epicondyle. When the condition becomes chronic, the inflammatory process dissipates and what is left is degeneration of the fascia of the tendon; at that stage the term lateral epicondylitis is often replaced with lateral epicondylosis.
How is tennis elbow treated with massage?
Deep cross-fiber work at the tendon is especially valuable when the client is at the chronic osis stage, because it draws in new blood that can help to repair the degenerated fascial tissue. PRP injections may also be recommended for clients with fascial degeneration.
