Quick-Answer Summary
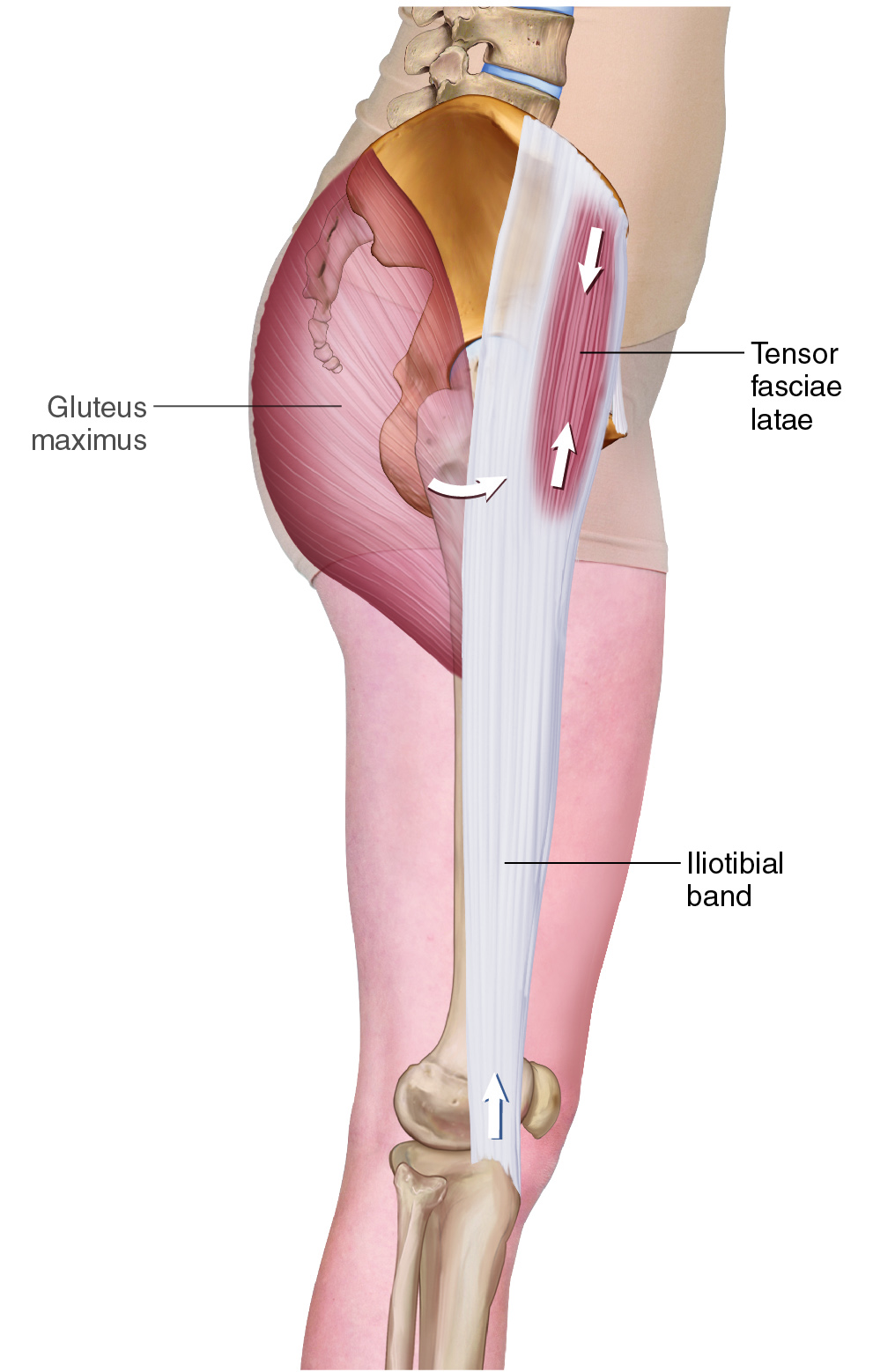
Lateral view of the right-side Tensor Fasciae Latae (TFL). (Permission: Dr. Joe Muscolino – learnmuscles.com)
What is the TFL? The TFL (tensor fasciae latae) is a hip flexor muscle in the anterolateral thigh that attaches from the ASIS to the iliotibial band (ITB). It performs hip flexion, abduction, and medial rotation (open-chain) and anteriorly tilts the pelvis (closed-chain). It is commonly tight, strongly linked to lower crossed syndrome, and is a key target for massage and stretching.
Introduction
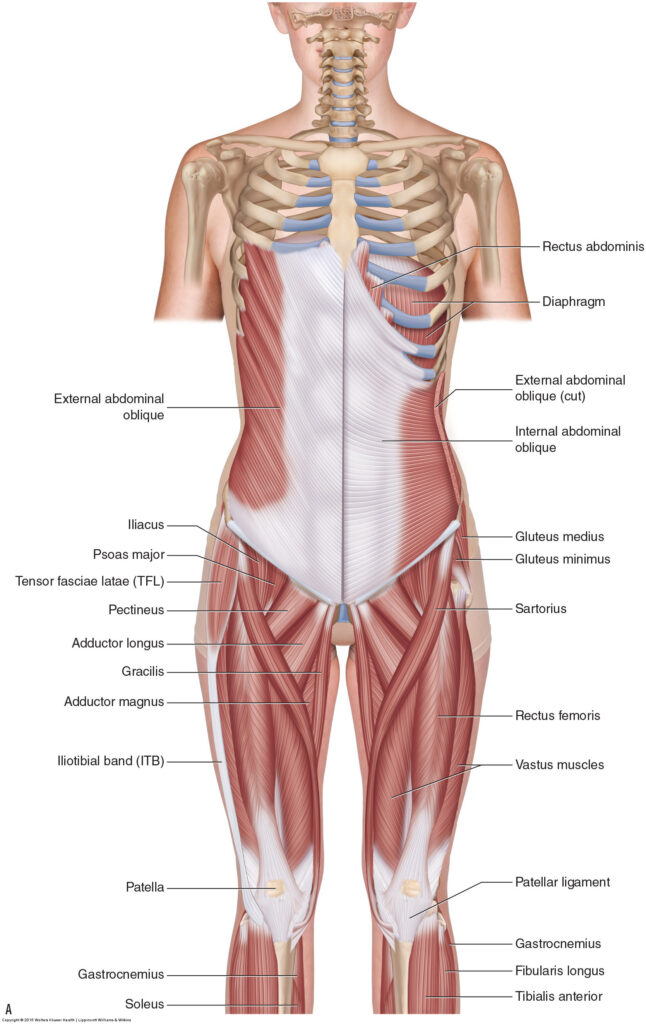
Superficial anterior view of the hip flexor functional group (permission: Dr. Joe Muscolino)
The tensor fasciae latae (TFL) is a muscle in the anterolateral thigh. It is part of the hip flexor group, as well as having other joint actions. The hip flexors are an important functional group of musculature to know and be able to assess and treat because of their involvement in a postural distortion pattern known as lower crossed syndrome. And the TFL itself is specifically important because it is often tight and painful in clients.
TFL Attachments
The TFL attaches proximally (origin) onto the ASIS and distally (insertion) into the iliotibial band (ITB) of the thigh.
More specifically, it attaches proximally from the:
ASIS and anterior iliac crest
to the
ITB, approximately ¼ of the way down the thigh.
| Attachment | Location |
|---|---|
| Proximal (Origin) | ASIS and anterior iliac crest |
| Distal (Insertion) | Iliotibial band (ITB), ~¼ down the thigh |
TFL Joint Actions/Functions
The TFL crosses the hip joint, so it has its joint actions at the hip joint. Let’s explore these joint action functions first open-chain, then closed-chain.
Open-Chain Joint Actions
Open-chain movements occur when the pelvis is fixed and the femur (thigh) is mobile and moves toward the pelvis. In other words, distal attachment (insertion) moves toward proximal attachment (origin). These are what could be described as the typically-thought-of, standard joint actions.
- The TFL crosses the hip joint anteriorly in the sagittal plane, so it flexes the thigh at the hip joint.
- The TFL crosses the hip joint laterally in the frontal plane, so it abducts the thigh at the hip joint.
- The TFL also wraps around the femur in the transverse plane such that it medially (internally) rotates the thigh at the hip joint.
BUT… The TFL has only one line of pull, so it cannot do any of these isolated cardinal-plane joint actions; rather, it must pull across all three planes to perform a multiplane/oblique-plane motion pattern that is a combination of all three of the joint actions. In other words, we might say (although this is not allowed in standard kinesiology terminology) that the TFL “flexo-abducto-medially rotates” the thigh at the hip joint 🙂
Closed-Chain Joint Actions
In closed-chain, the distal end of the lower extremity is fixed, so the thigh is fixed, so the pelvis moves toward the thigh at the hip joint (instead of the thigh moving toward the pelvis). It should be noted that during the gait cycle, the foot is on the ground (and therefore essentially fixed/stabilized) 60% of the time, so in the lower extremity, closed-chain joint motions are often more common than open-chain ones. And, in standing posture, for example when you might be assessing the client’s posture, the feet are on the floor, so essentially fixed, so the pull from hip joint musculature would play out upon the pelvis (except perhaps transverse-plane rotations), so the client’s pelvic posture would demonstrate the balance of the hip joint musculature. And, given that the posture of the pelvis determines the posture of the spine, we can see how important assessing and treating hip joint musculature is!
For example, if hip flexors are tighter than hip extensors, the client will have an excessively anteriorly tilted pelvis. If the hip extensors are tighter than hip flexors, the client will have a posteriorly tilted pelvis. etc.
So, now, looking at the cardinal plane closed-chain joint actions of the TFL at the hip joint…
- The TFL crosses the hip joint anteriorly, so in closed-chain, the pelvis anteriorly tilts in the sagittal plane toward the femur at the hip joint.
- The TFL crosses the hip joint laterally, so in closed-chain, the pelvis depresses (laterally tilts) in the frontal plane toward the femur on that side at the hip joint.
- The TFL crosses the hip joint in the transverse plane such that the pelvis ipsilaterally rotates in the transverse plane toward the femur at the hip joint.
But, the TFL has one line of pull, so it must pull across all three planes such that it would create an oblique-plane motion pattern that is a combination of anterior tilt, same-side depression, and ipsilateral (same-side) rotation of the pelvis at the hip joint.
Note: Because the TFL attaches into the ITB, which crosses the knee joint anterolaterally, the TFL’s contractile pulling force would help to extend the knee joint and stabilize the knee joint laterally.
Nearby Anatomy
Superficial anterior view of the hip flexor functional group (Permission: Dr. Joe Muscolino)
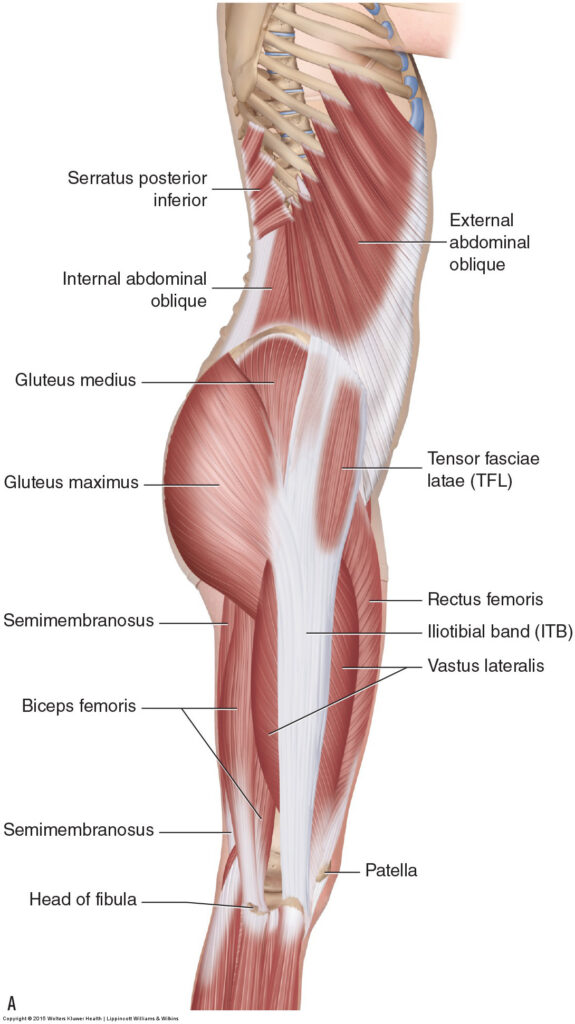
Superficial right-lateral view of the gluteal/thigh region (Permission: Dr. Joe Muscolino)
The TFL is one of two muscles that attach onto the ASIS; the other is the sartorius. Immediately medial to the TFL are the sartorius and the rectus femoris of the quadriceps femoris group. Immediately lateral to the TFL (and also deep to its lateral aspect) is the gluteus medius, and deep to that, the gluteus minimus. And, as the TFL runs distally, it is superficial to the vastus lateralis of the quadriceps group.
TFL and Lower Crossed Syndrome
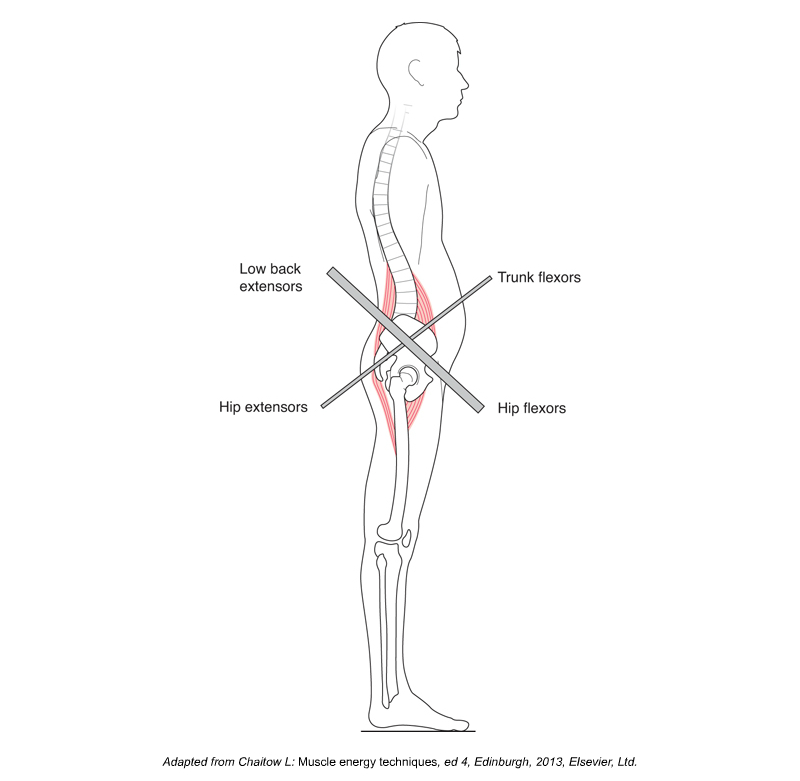
Lower crossed syndrome (LCS). Permission Dr. Joe Muscolino – Kinesiology textbook 4th ed.
The TFL is one of the muscles of the hip flexor functional group, so it is extremely important because of the relationship between tight hip flexors and a postural distortion pattern known as lower crossed syndrome (LCS). This condition was named by the Czech physiologist, Vladimir Janda. LCS is marked by excessive anterior tilt of the pelvis, which in turn results in the sacral base angle being excessive, which then results in hyperlordosis (hyperextension) of the lumbar spine. This can cause jamming of the facet joints, which can cause low back pain and dysfunction.
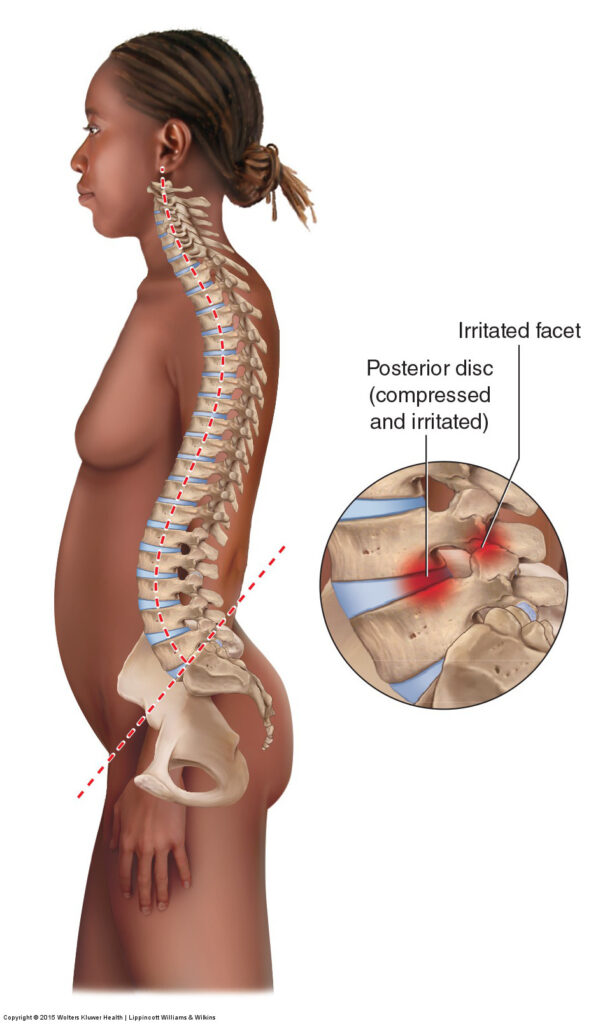
Excessive pelvic anterior tilt with the sacral base angle excessive, resulting in hyperlordosis of the lumbar spine. Permission Dr. Joe Muscolino – learnmuscles.com.
The principal reason that the pelvis would be in excessive anterior tilt is that the muscles of anterior tilt at baseline tone are tighter (overly facilitated) compared to the muscles of posterior tilt (overly inhibited). The primary muscles of anterior tilt are the hip flexor muscles (thigh flexion is the open-chain action of closed-chain pelvic anterior tilt). Thus, we have the hip flexor group locked-short, and the hip extensor group (primarily the posterior gluteal fibers) locked long. The other two muscle groups that could contribute to excessive anterior tilt of the pelvis would be the trunk flexors (posterior tilters) and low back extensors (anterior tilters).
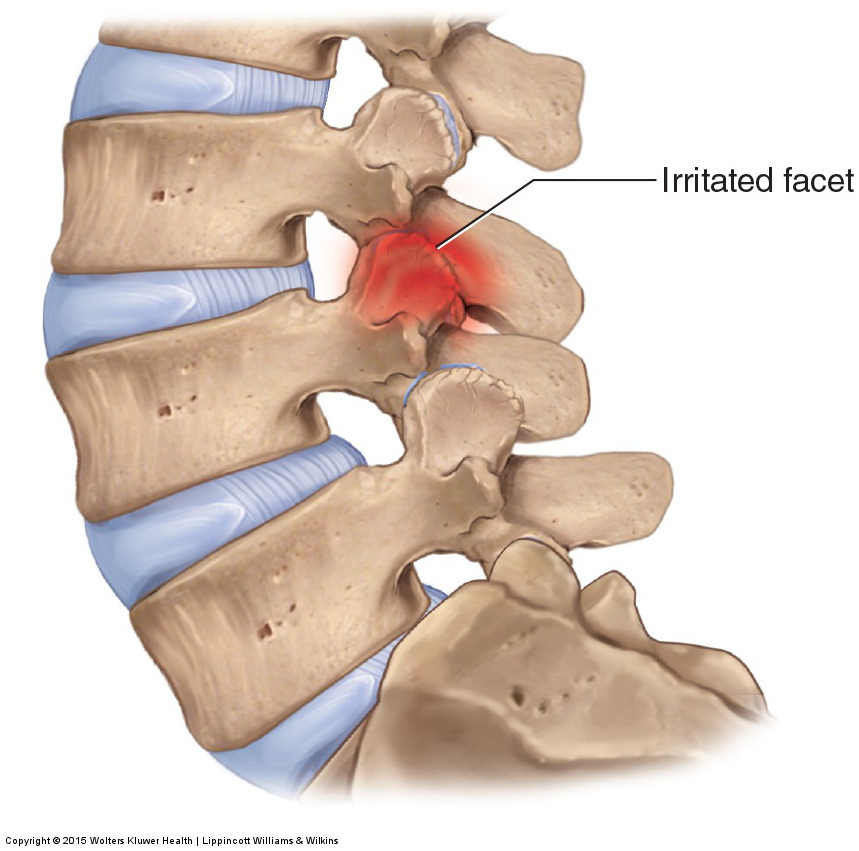
Hyperlordosis (excessive extension) of the lumbar spine shifts weight posteriorly onto the facets, which can cause low back pain and dysfunction. Permission Dr. Joe Muscolino – learnmuscles.com.
Why might the hip flexor functional group be overly facilitated and tight? One reason is that we sit so much during the day. When we sit, the hip flexors are shortened. Then, by the principal of adaptive shortening, they become tighter. For this reason, it is so valuable to be competent at assessing and treating the hip flexor group, including the TFL.
Palpating the TFL

Palpation of the right TFL. Permission Dr. Joe Muscolino – Muscle and Bone Palpation Manual, 3ed.
The TFL is extremely easy to palpate because we can use the ASIS as a landmark. With the client supine, find the ASIS, and then drop immediately distal and a bit lateral. You will be on the TFL. Now ask the client to medially rotate the thigh and slightly lift it up into flexion. You will feel the TFL engage and pop. Strum perpendicular across it (horizontally) from its medial border to its lateral border. Now, drop a baby step more distally (keeping in line how it runs a bit laterally as it runs distally), and repeat this process of having the client contract and relax the TFL; feel for it to harden and strum perpendicularly across it, and then feel for it to soften when they relax it.
I like to say that when your target muscle engages, if you are able to isolate its contraction, it will be the only hard, soft tissue, amongst a sea of soft, soft tissues.
Now that you have located the TFL, assess it at baseline tone for any tightness/tautness, whether it be global tightness, focal myofascial trigger points (TrPs), or fibrous adhesions. The TFL is often tight, probably because it is contained within the fibrous fascial tissue of the ITB, so careful assessment and methodical deliberate soft tissue work and stretching is extremely valuable.
Note: In the accompanying illustration, the client is positioned with their right thigh on the table, and their right (lower) leg hanging off the table (their left hip and knee should be flexed with their left foot on the table to stabilize the pelvis, but is not shown so that the reader’s view would be less obstructed). This is a ideal position to palpate the musculature of the hip flexor group because it allows for isolated engagement of hip joint muscles versus knee joint muscles. But, if used, the client should NOT remain in this position for a prolonged period of time because the pelvis is not fully stabilized, so low back pain can occur.
Stretching the TFL
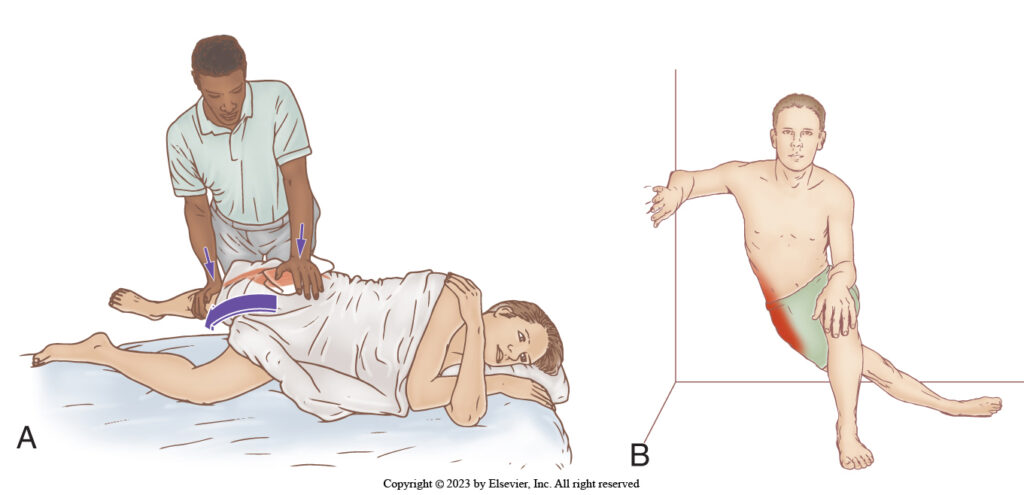
Stretching the right-side TFL: Therapist-assisted with the client side-lying and diagonally oriented on the table; and client self-care. Permission: Dr. Joe Muscolino – The Muscle and Bone Palpation Manual, 3ed.
The TFL is most effectively stretched with the client side-lying on the opposite side of the TFL that you will be stretching. So, for example, to stretch the right-side TFL, have the client lying on their left side, positioned diagonally so that their left shoulder is far from you, and their pelvis is close to the side where you are standing. The object of the stretch is to drop their right thigh down toward the floor into adduction (they are positioned diagonally so that the table will not obstruct the excursion of the thigh down into adduction). First, make sure that their lumbar spine is “stacked” (i.e., there is no rotation). Place your left hand on their iliac crest and introduce the stabilization force toward elevation of their pelvis to prevent their pelvis from dropping into depression when the stretch is performed (place a cushion between your hand and their iliac crest for their comfort). Now, with your right-hand contact on their distal lateral thigh (do not cross their knee joint to contact their [lower] leg because that would place a frontal-plane torque into their knee joint), and slowly bring their right thigh into adduction toward the floor to stretch the TFL.
Massaging the TFL
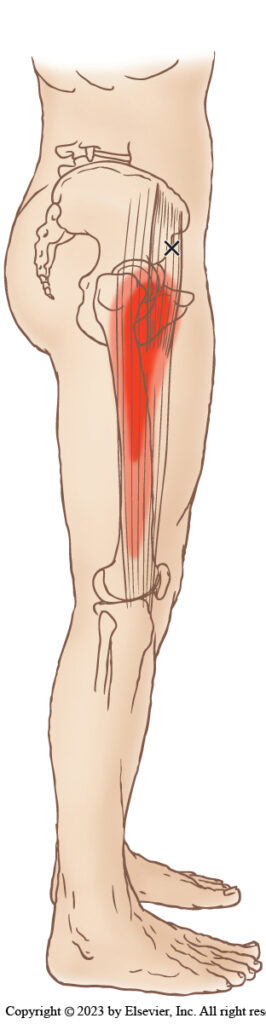
Common TrPs and their referral zones for the right-side TFL. Permission: Dr. Joe Muscolino – The Muscle and Bone Palpation Manual, 3rd ed.
Massaging the TFL is extremely valuable because it is so often tight and so often has TrPs. The TFL can be easily worked with the client side-lying or supine. Massage and heat should always be done before stretching because this warms the tissue so that the stretch procedure is safe and more effective.
Conclusion
Understanding the role that the TFL can play with lower crossed syndrome (LCS) is crucial toward assessing and treating clients who present with this postural distortion pattern. Beyond LCS, knowing how to assess and treat the TFL is important in its own right because the TFL is so often tight and painful.

Dr. Joe Muscolino
Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com,
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
