What is the piriformis muscle, and why does it matter in manual therapy?
Introduction
In the world of manual therapy, the piriformis is considered to be one of the most important muscles in the human body. As a member of the deep lateral rotator group, it is involved in hip joint function and dysfunction. And because it attaches on to the sacrum, it effectively crosses the sacroiliac joint so it is also involved in sacroiliac function and dysfunction. The piriformis is also a fascinating muscle because with a change in joint angle, its function at the hip joint changes.
Piriformis Attachments
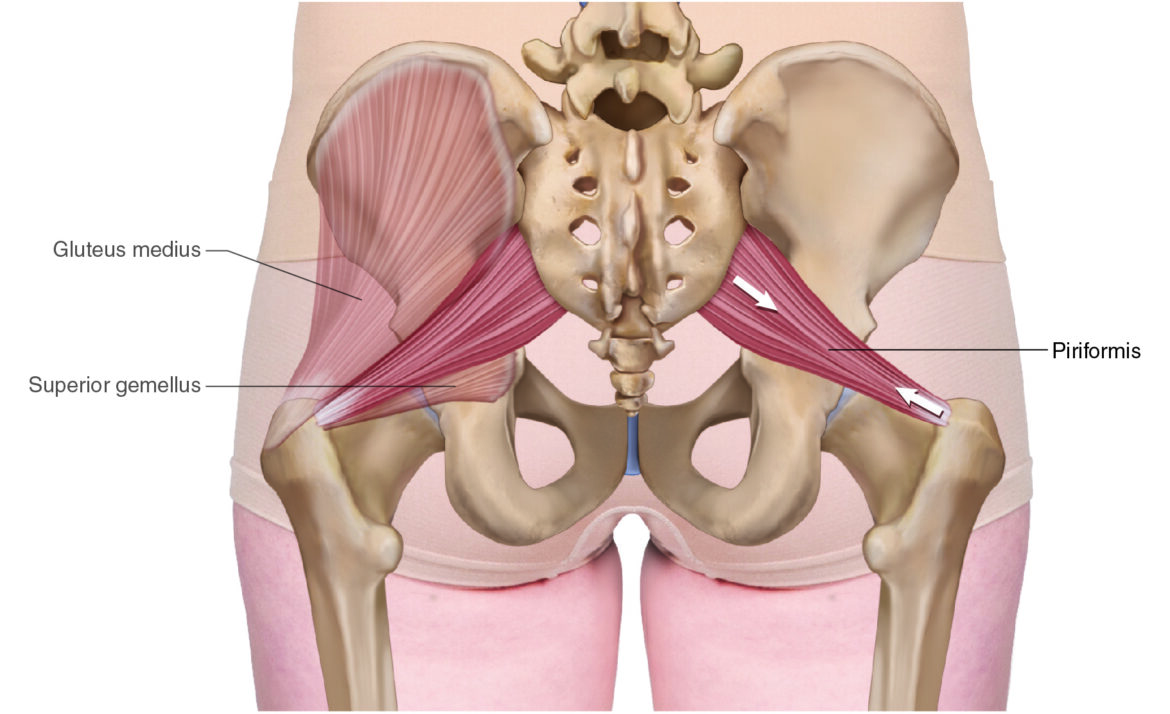
The piriformis attaches proximally onto the sacrum (origin) and distally onto the greater trochanter of the femur (insertion).
More specifically, it runs from…
- the anterior aspect of the sacrum (levels S2–S4)
to the
- superior aspect of the greater trochanter of the femur
Quick Answer: The piriformis attaches proximally onto the anterior sacrum (S2–S4) and attaches distally onto the superior greater trochanter of the femur.
Piriformis Functions
Open-Chain
The piriformis crosses the hip joint, therefore it has function at the hip joint. When in anatomic position, it crosses the hip joint posteriorly with a horizontal direction to its line of pull, therefore the piriformis laterally rotates the thigh at the hip joint. The piriformis can also contribute to abduction of the thigh at the hip joint.
However, if the thigh (femur) is first flexed 60 degrees or more (let’s picture it flexed to 90 degrees), its line of pull moves to the other side of the axis for motion in the transverse plane, so the piriformis becomes a medial rotator of the thigh at the hip joint.
Even if the therapist does not consciously realize this, there is a reason that it should be intuitively known… because the popular Figure-4 stretch for the piriformis is performed by laterally rotating the (flexed) thigh at the hip joint… And given that a stretch lengthens a muscle, if the lateral rotation of the Figure-4 stretch is the opposite of the piriformis’s joint action, then the piriformis must be a medial rotator of the thigh.
When the thigh is first flexed at the hip joint, the piriformis can also horizontally abduct the thigh at the hip joint.
This all becomes important when we are stretching the piriformis because if we know the piriformis’ joint action (in any given position), then we can figure out how to stretch it… Simply do the opposite.
This conversation is open-chain mechanics in which the distal attachment is free to move, so it moves toward the proximal attachment. In other words, the thigh moves at the hip joint toward the sacrum (pelvis).
Quick Answer: In open-chain mechanics, the piriformis laterally rotates the thigh when the hip is in anatomic position, and becomes a medial rotator when the hip is flexed to 60° or more.
Closed-Chain
However, when the body is in closed-chain mechanics, in other words, the distal attachment is fixed, likely because the foot is stable against the ground, then the proximal attachment moves instead, i.e., the sacrum (pelvis) moves at the hip joint toward the thigh. This closed-chain (also known as reverse action) for lateral rotation of the thigh is contralateral rotation of the pelvis at the hip joint. So…
The piriformis contralaterally rotates the pelvis at the hip joint.
This is actually a very common movement of the body. When we are walking or running and we plant a foot on the ground and we want to change our direction (referred to as planting and cutting), we have a stable/fixed foot, and therefore the thigh is stable/fixed, so the pelvis moves instead.
The closed-chain movement for lateral rotation of the thigh at the hip joint is contralateral rotation of the pelvis at the hip joint.
Note: This is one of the reasons that there is more “lateral rotation musculature” in the body than “medial rotation musculature”… not to laterally rotate the thigh, but to contralaterally rotate the pelvis!
Quick Answer: In closed-chain mechanics (e.g., when the foot is planted), the piriformis contralaterally rotates the pelvis at the hip joint — a key function during walking/running and changing direction (planting and cutting) movements.
Nearby Anatomy
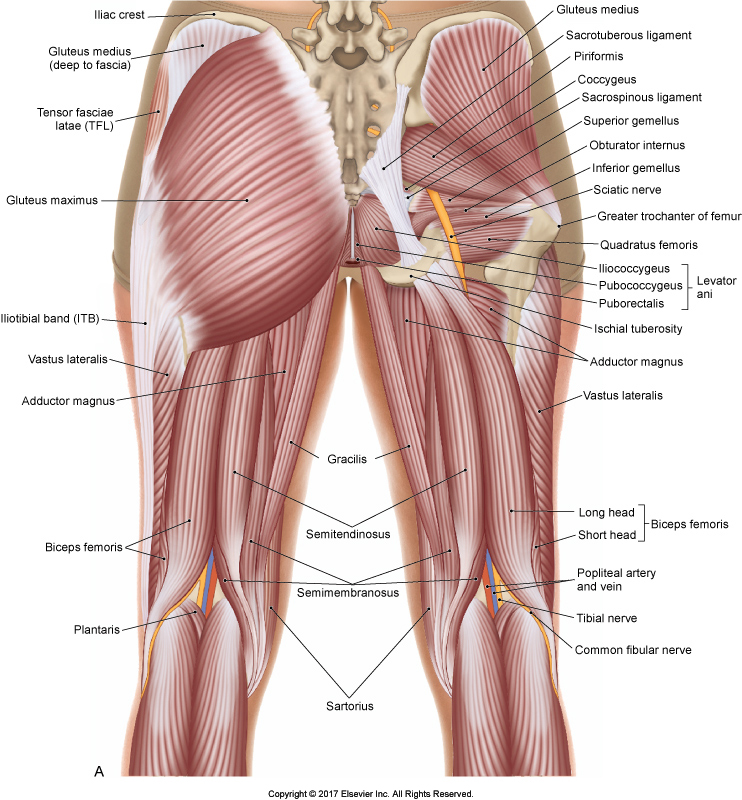
Posterior view of the pelvis. Permission Dr. Joe Muscolino – The Muscular System Manual 5ed.
The piriformis is deep to the gluteus maximus. The piriformis is the most superior (proximal) member of the deep lateral rotator group; immediately inferior (distal) to the piriformis is the superior gemellus. Superior (proximal) to the piriformis is the gluteus medius. The sciatic nerve usually enters the gluteal region through the greater sciatic foramen, between the piriformis and the superior gemellus. There are variants in which the sciatic nerve, or a part of it (usually the common fibular nerve portion) pierces directly through the piriformis.
Key anatomic relationships of the piriformis:
- Deep to the gluteus maximus
- Inferior to the gluteus medius
- Superior to the superior gemellus
- Adjacent to the sciatic nerve (passing through the greater sciatic foramen)
Piriformis Syndrome
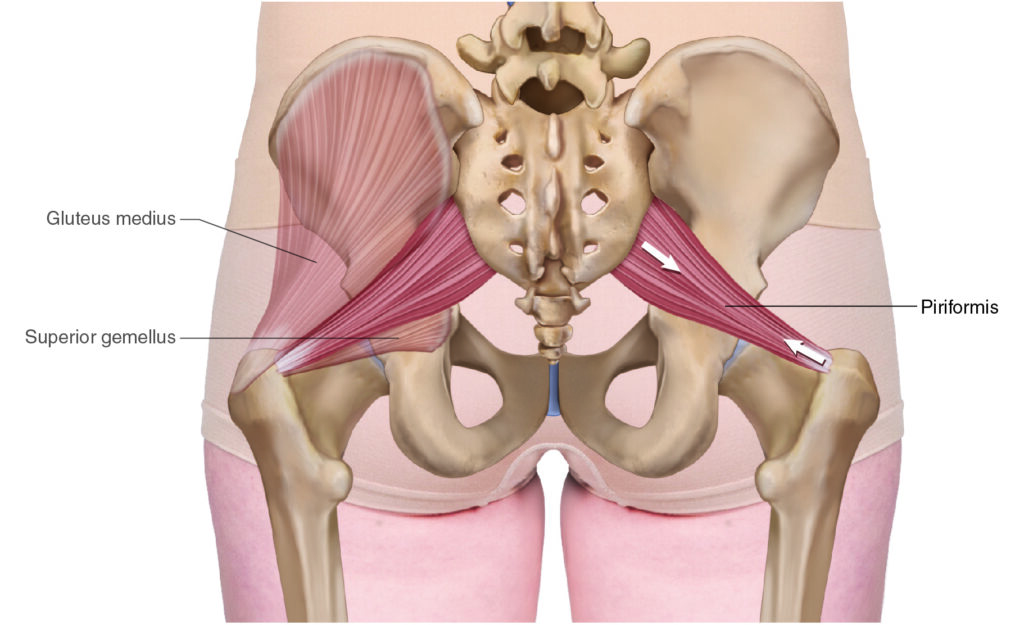
Piriformis. Permission Dr. Joe Muscolino (learnmuscles.com).
What is Piriformis Syndrome?
The sciatic nerve. Permission Dr. Joe Muscolino (learnmuscles.com).
Because of the proximity of the sciatic nerve, regardless of whether it passes between the piriformis and superior gemellus or directly through the piriformis, a tight piriformis can cause compression of the sciatic nerve. When this occurs, it is called piriformis syndrome, which is a form of sciatica. The symptoms would be essentially identical to sciatica caused by nerve root compression in the intervertebral foramina of the spine.
Note: Sometimes sciatica caused by compression of the sciatic nerve by a tight piriformis muscle is referred to as pseudo-sciatica. However, compression of the sciatic nerve caused by any structure is technically sciatica.
Quick Answer: Piriformis syndrome occurs when a tight piriformis muscle compresses the sciatic nerve, producing symptoms essentially identical to lumbar-origin sciatica.
Palpating the Piriformis

Piriformis palpation. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
To palpate the piriformis, have the client prone. Find the midpoint between the PSIS and the sacrococcygeal joint line; then drop immediately off the sacrum. Now find the superior aspect of the greater trochanter. The piriformis can be palpated between these two points.
To engage the piriformis to make it contract and harden, flex the client’s (lower) leg at the knee joint, and with your contact on their distal medial leg (immediately proximal to the ankle joint), ask the client to try to gently laterally rotate their thigh against your resistance.
Feel for the piriformis to engage and pop, and strum perpendicularly across it. Then have the client relax and move your contact a baby step along the muscle, closer to the greater trochanter attachment. Have the client engage the piriformis again and palpate by strumming perpendicularly again. Repeat this protocol until you reach the greater trochanter attachment. Once the entire piriformis has been located, have the client fully relaxed and assess it by palpating the baseline tone of the piriformis.
Stretching the Piriformis
What are the best piriformis stretches?
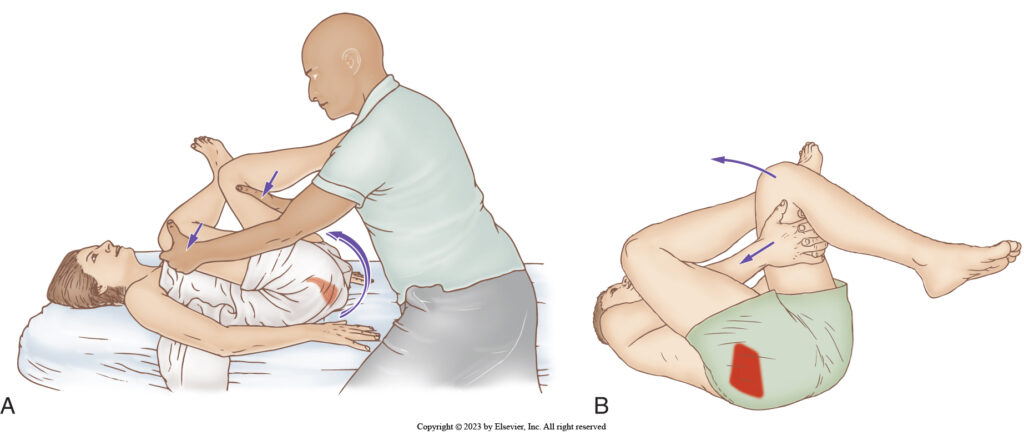
Figure-4 stretch for the piriformis: therapist-assisted and client self-care. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
There are many stretching protocols for the piriformis. But caution should be exercised with any of them that place a torque into the knee joint. So, before the stretching protocol, be sure that the client’s knee is healthy; and during the stretch, confirm this by making sure that the client does not feel any knee pain or discomfort during the protocol.
Figure-4 Stretch
The most common stretch protocol, and likely the most effective, is the Figure-4 stretch with the client supine. However, this stretch does torque the knee so it is contraindicated if the client has an unhealthy knee.

Figure-4 piriformis stretch with increased rotation added by pulling back on the client’s right knee as their left foot is pushed toward their body. Permission Dr. Joe Muscolino (learnmuscles.com).
One amendment to carrying out the Figure-4 stretch compared to the first two illustrations is that instead of pushing the client’s right thigh with your left hand, you can pull toward you instead (see illustration immediately above). This increases the rotation force into the stretch and is more powerful. Similarly, with the client self-care version, the client can re-place their right hand on their distal anterior right thigh and push the thigh away, thereby increasing the stretch force with this protocol.
Horizontal Adduction Stretch

Horizontal adduction stretch – Ipsilateral stance, pushing the thigh into horizontal adduction. Permission Dr. Joe Muscolino (learnmuscles.com).
The horizontal adduction stretch is performed with the client supine and their knee and hip joints flexed to approximately 90 degrees. Their thigh is then brought toward the opposite side of their body, into horizontal adduction. To avoid compression and/or torquing their knee, be sure to contact on their distal lateral thigh and not distal to the knee joint on their (lower) leg. There are a number of ways to perform this stretch. The accompanying illustrations demonstrate some of your choices.

Horizontal adduction stretch with contralateral stance and pulling their thigh into horizontal adduction. Permission Dr. Joe Muscolino (learnmuscles.com).
Although this stretch can successfully avoid torquing the knee, it can cause compression and pinching pain in the client’s proximal anterior thigh (at the inguinal ligament area), usually caused by compression of their hip flexor musculature (or perhaps restriction in the hip joint causing jamming of the femur into the acetabulum). If this occurs, then it is helpful to first loosen the hip flexor musculature (via heat, massage and stretching) before stretching the piriformis. And if it the anterior pinching pain is caused by hypomobile joint dysfunction of the hip joint, then Grade IV slow-oscillation joint mobilization can relieve the restriction and pain.

Tractioning hip flexor tissue to decrease anterior hip pinching pain with horizontal adduction stretch. Permission Dr. Joe Muscolino (learnmuscles.com).
If the pinching pain persists and interferes with your ability to perform the piriformis stretching protocol, then there is a method to open up and traction the anterior hip as seen in the illustration above.
Quick Answer: The two primary piriformis stretches are the Figure-4 stretch (supine) and the horizontal adduction stretch. The Figure-4 is contraindicated for clients with knee issues.
Massaging the Piriformis
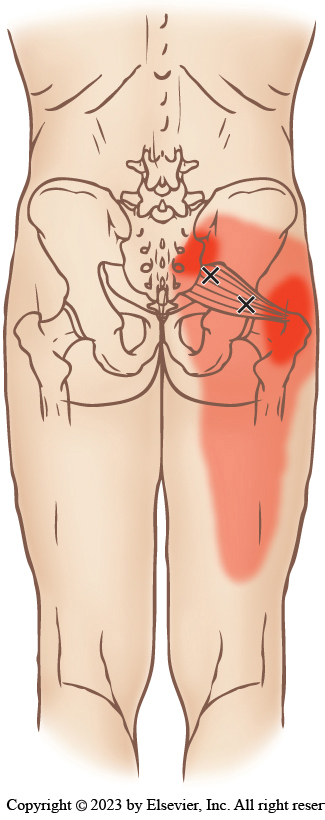
Piriformis trigger points and their referral zones. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
How do you massage the piriformis muscle?
Even though the piriformis is deep to the gluteus maximus, it can usually be easily massaged because the gluteus maximus in most clients is not very tight at baseline tone. If you are working through the sheet (or clothing), then working the piriformis ipsilaterally (from the same side of the table) is usually best. If you are using lotion/oil for Swedish strokes, then standing on the opposite side of the table (contralaterally) is usually best with the stroke running from the medial to lateral (sacrum toward femur). If the strokes are perpendicularly (transversely) across the muscle, then standing ipsilaterally works fine.
Conclusion
The piriformis is an extremely important muscle with which manual therapists should be comfortable and efficient working because of its role in hip and sacroiliac joint function and dysfunction. The classic approach of heat, massage, and stretching can be very beneficial for clients.
Frequently Asked Questions About the Piriformis Muscle
What does the piriformis muscle do? The piriformis laterally rotates the thigh at the hip joint when the hip is in anatomic position. When the hip is flexed to 60° or more, it becomes a medial rotator. In closed-chain movement, it contralaterally rotates the pelvis.
Where does the piriformis attach? The piriformis attaches proximally (originates) at the anterior sacrum (S2–S4) and attaches distally (inserts) onto the superior aspect of the greater trochanter of the femur.
What is piriformis syndrome? Piriformis syndrome is compression of the sciatic nerve by a tight/hypertonic piriformis muscle, producing sciatica symptoms including gluteal and thigh/leg pain.
What is the best stretch for the piriformis? The figure-4 stretch (supine) is widely considered the most effective piriformis stretch, though it is contraindicated for clients with knee joint issues. The horizontal adduction stretch is a safer alternative.
How do you palpate the piriformis? With the client prone, locate the midpoint between the PSIS and sacrococcygeal joint line, drop off the sacrum, and identify the superior greater trochanter. The piriformis is palpable between these landmarks.
Biography

Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com.
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
