Permission Dr. Joe Muscolino (learnmuscles.com).
Quick Answer: The supraspinatus muscle cannot perform (pure) frontal-plane abduction. Instead, it creates an oblique-plane motion called scaption — approximately 2/3 abduction and 1/3 flexion — in the plane of the scapula. This distinction matters not only for accurate palpation of the supraspinatus, but also for the larger concept of how muscles function.
Introduction
The supraspinatus is one of the four rotator cuff muscles and is named for being located in the supraspinous fossa above the spine of the scapula. The major joint action of the supraspinatus is abduction of the arm at the shoulder joint, but if you were to ask what motion pattern the supraspinatus creates when it contracts and shortens, frontal-plane abduction of the arm at the shoulder joint would not be the answer? Huh? Read on to understand what this means.
In addition to this, the supraspinatus is often involved in the condition known as shoulder impingement syndrome.
Supraspinatus Attachments
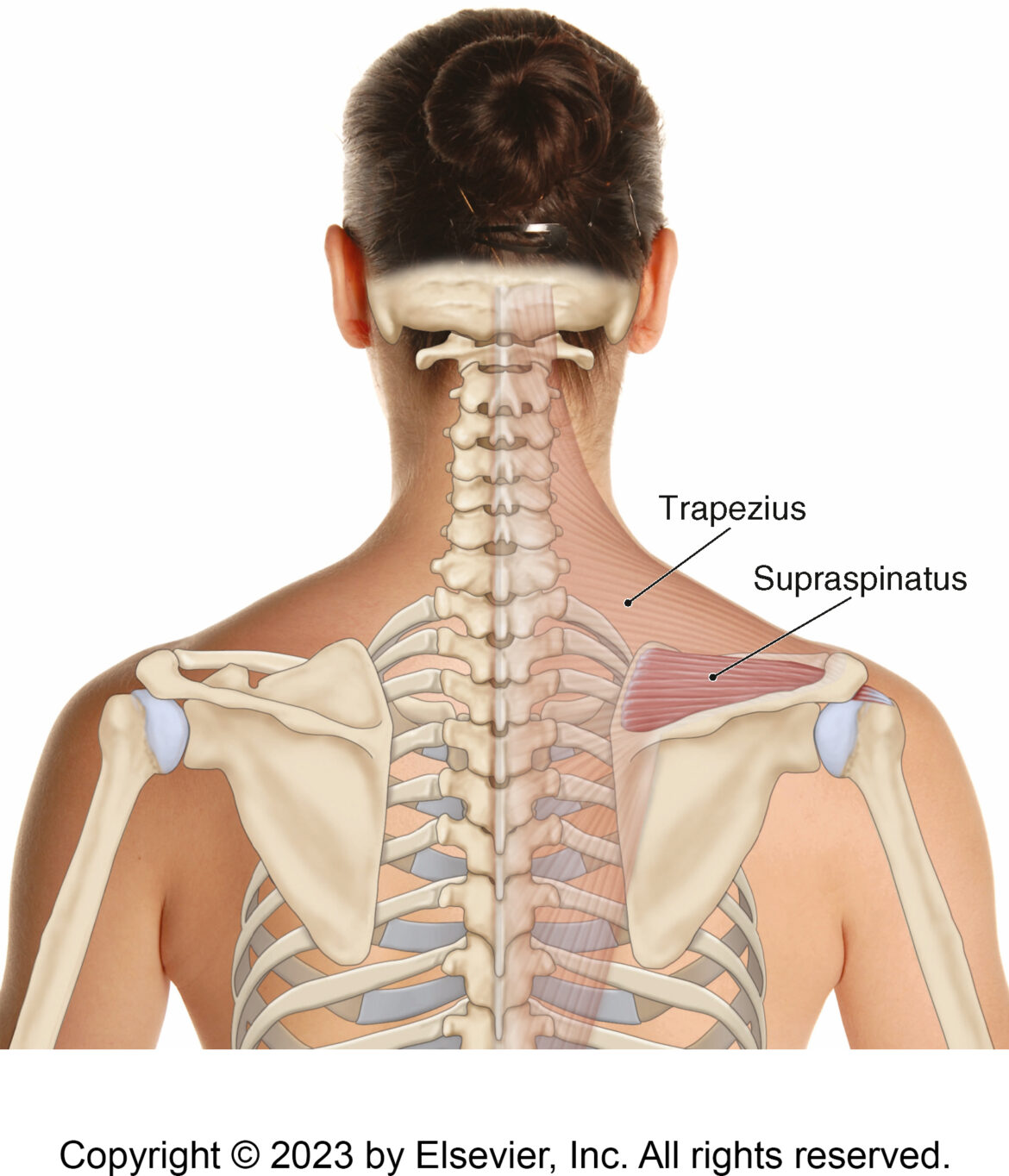
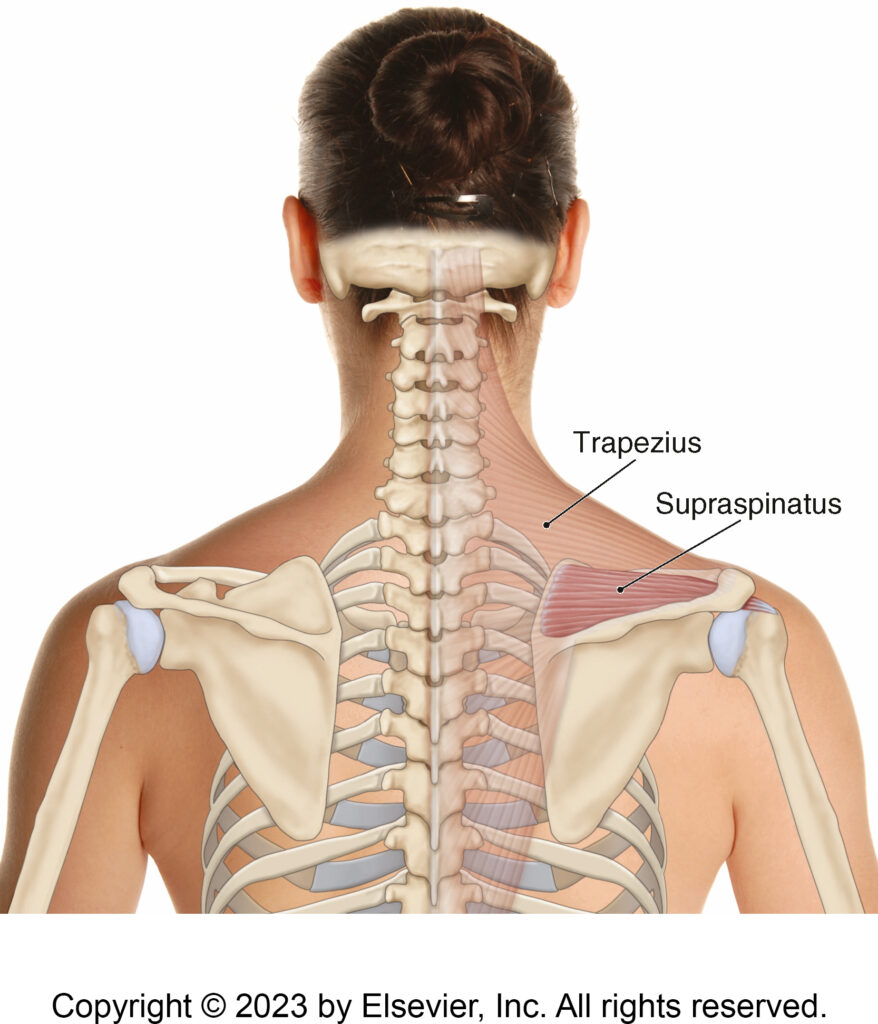
The supraspinatus attaches proximally into the supraspinous fossa of the scapula, just above the spine of the scapula (origin). From there, it runs deep to the acromion process of the scapula to arrive at its distal attachment on the greater tubercle on the head of the humerus (insertion).
More specifically, the supraspinatus attaches from the…
- medial 2/3 of the supraspinous fossa
to the
- superior facet of the greater tubercle
Supraspinatus Functions
Abductoflexion…
The supraspinatus crosses the glenohumeral (GH/shoulder) joint with a vertical line of force as it travels down to the head of the humerus. It is important to note that the path of the supraspinatus is not in the frontal plane; it is in the plane of the scapula.
This means that the movement created by the supraspinatus, is not in the frontal plane, but rather is in the plane of the scapula, an oblique plane which is approximately 30 degrees off the frontal plane toward the sagittal plane. However, joint actions are, by definition (with a few rare exceptions), cardinal-plane movements. When a muscle creates a movement in an oblique plane, kinesiology terminology is not set up to name these oblique-plane movements. If it were, we would say that the supraspinatus “abductoflexes” the arm at the shoulder joint. Instead, the muscle’s function must be described by breaking it down into its cardinal-plane components. So, a muscle atlas (that is complete) will state that the supraspinatus abducts and flexes the arm at the shoulder joint. But the problem is that this leads the student/therapist to believe that the supraspinatus can do abduction, or that it can do flexion; it cannot do either joint action by itself. At least it cannot do pure abduction in the frontal plane or pure flexion in the sagittal plane. This is why the title of this blog is “Supraspinatus Cannot Abduct the Arm“.
The supraspinatus has one line of pull, and that line of pull is across both cardinal planes, so it must create one oblique-plane motion that is a combination of the two cardinal-plane joint actions. As stated, this means that the supraspinatus cannot do pure abduction of the arm, nor can it do pure flexion of the arm; it must do a combination of both together… abductoflexion.
Is this just trivia that is geeky and unimportant? No. It actually has practical importance to the world of manual therapy. This will be stated later in the palpation section, but to state it generally now, when we want to palpate a target muscle, what we usually do is ask the client to contract the muscle so that it hardens and we can discern it from adjacent musculature (if the target muscle’s contraction can be isolated, then it will be…
the only hard, soft tissue amongst a sea of soft, soft tissues.
So, during the supraspinatus palpation protocol, most therapists will ask the client to try to abduct the arm at the shoulder joint. Yes, this will engage the supraspinatus and be helpful. But, asking for an engagement in the plane of the scapula would actually create a better engagement of the supraspinatus because it is exactly what the muscle does when it contracts. So, asking for the oblique-plane motion that is a combination of abduction with some flexion will better engage the supraspinatus and create a more accurate palpation protocol.
Some sources describe this motion as scaption because it is in the plane of the scapula. With healthy ideal posture, this movement would be approximately 2/3 abduction and 1/3 flexion.
Full Range of Motion…
Another note regarding the function of the supraspinatus. It was believed many years ago that the supraspinatus could only initiate abduction of the arm at the shoulder joint; that it could not bring the arm through the full range of motion of abduction (or, more correctly, abductoflexion). This was disproven many decades ago, but it continues to be repeated, probably because current teachers learned from past teachers who learned from past teachers, etc., so the old incorrect belief lives on.
Like any muscle, the supraspinatus has the ability to contract until it reaches its maximum contracted short length (generally, a non-pennate muscle can contract to approximately half its resting length). But just because it can contract for the full range of motion of the arm, that does not necessarily mean that the nervous system will always go to the supraspinatus to engage for the full range of motion. The nervous system often chooses one muscle of a functional group over another for a specific phase of the range of joint motion. It just needs to be emphasized that the supraspinatus can create a full abduction/abductoflexion range of motion of the arm.
Having said this, when performing the supraspinatus palpation protocol, we do only ask for a small range of motion. But there is actually another specific reason for this. That will be discussed later the Palpation section.
Nearby Anatomy
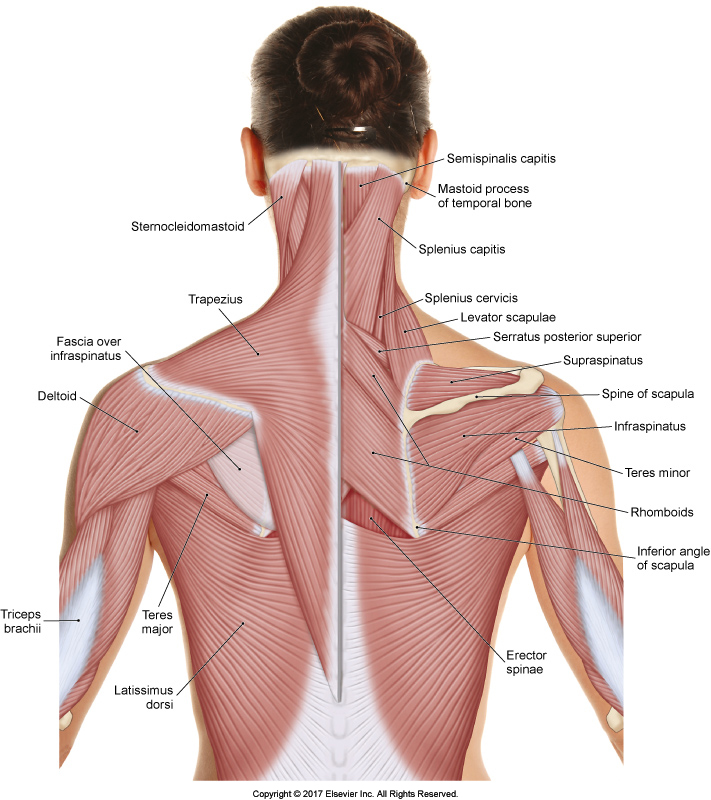
Permission Dr. Joe Muscolino – The Muscular System Manual 5ed.
The supraspinatus is located in the supraspinous fossa of the scapula; the infraspinatus is in the infraspinous fossa. Directly medial and a bit superior to the supraspinatus is the levator scapulae attachment on the scapula.
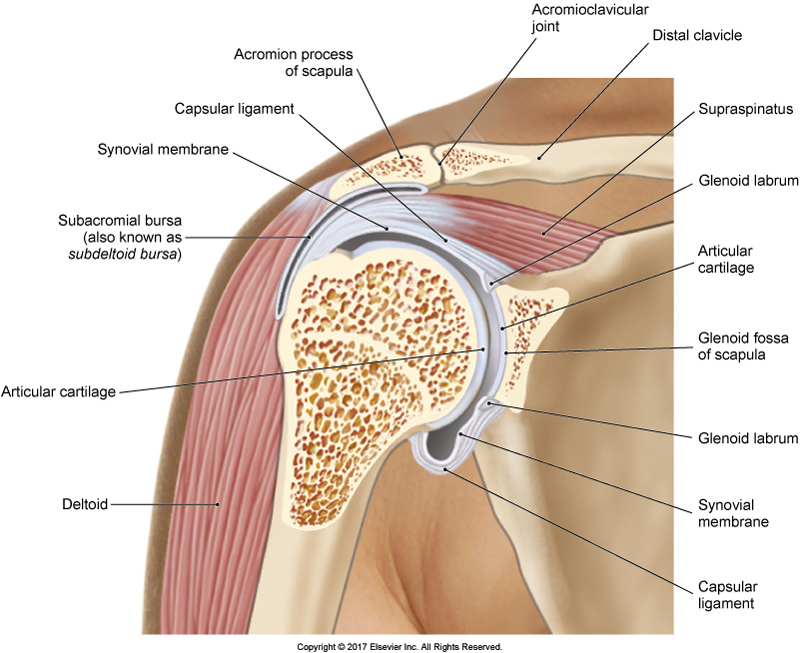
The belly of the supraspinatus is deep to the upper trapezius; the distal tendon of the supraspinatus is deep to the deltoid. The distal tendon is located between the head of the humerus and the acromion process above; this is a common site of compression/impingement. Between the supraspinatus distal tendon and head of the humerus is the subdeltoid (also known as the subacromial) bursa. On the greater tubercle of the scapula, the supraspinatus attachment lies next to, and usually blends into, the distal attachment of the infraspinatus.
Palpating the Supraspinatus
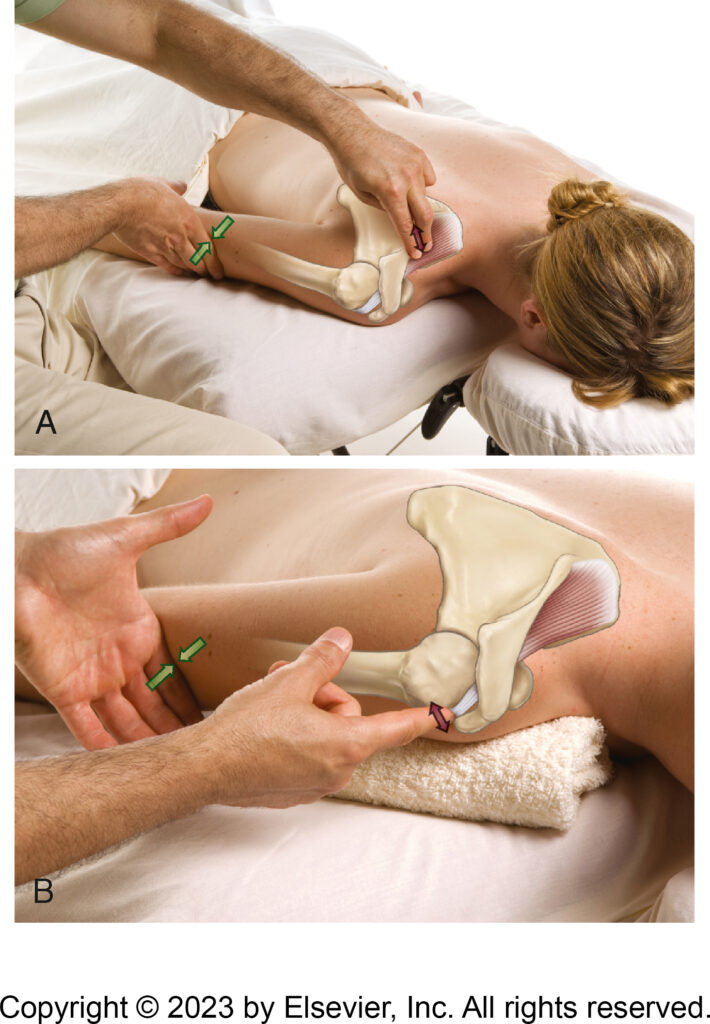
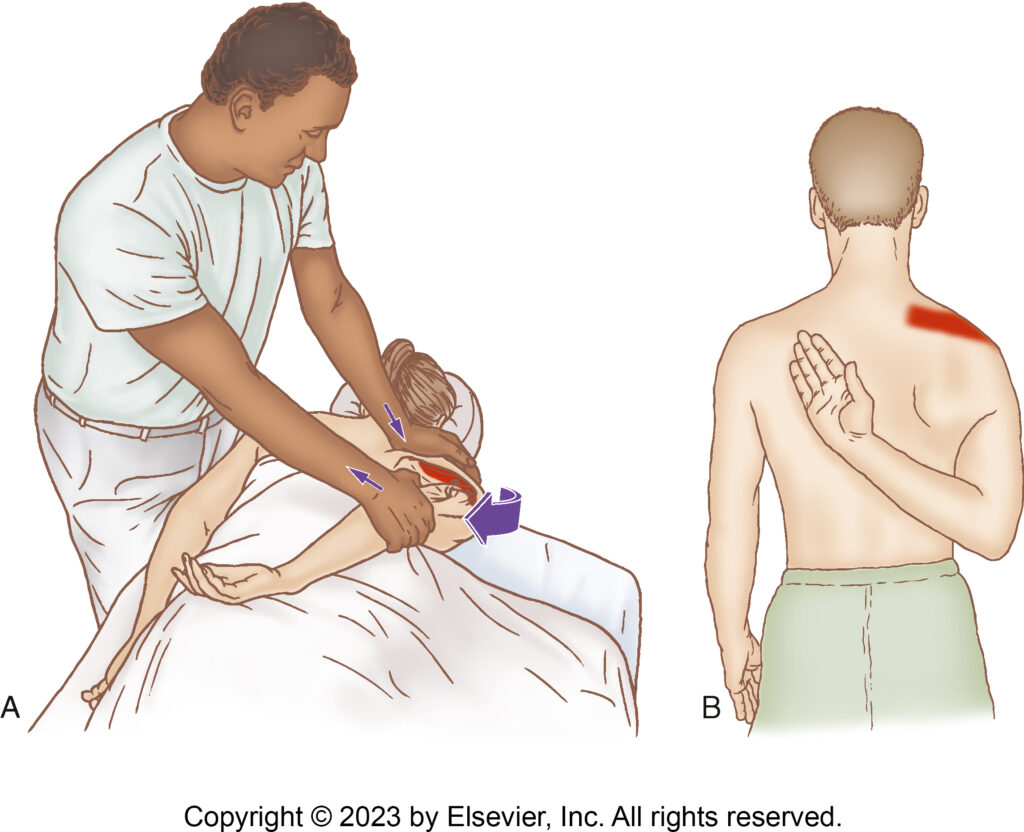
Palpation of the supraspinatus. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The belly of the supraspinatus lies deep to the upper trapezius; but can usually be successfully palpated by inhibiting the upper trapezius. This is accomplished by asking the client to place their hand in the small of the back (not seen in the accompanying photo). This requires extension and adduction of the arm at the shoulder joint, which via scapulohumeral rhythm requires downward rotation of the scapula. Because the upper trapezius is an upward scapular rotator, it is inhibited (due to the neural reflex known as reciprocal inhibition).
Find the spine of the scapula; and place your palpating finger pads immediately superior and you will be on the supraspinatus (deep to the upper trapezius). Now ask the client to perform a small abduction range of motion of the arm (perhaps 10-20 degrees), and feel for the engagement of the supraspinatus deep to the upper trap.

Palpating the supraspinatus with scaption. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
Note: If the client is seated, then asking for the arm to move into scaption is better than simply abduction for engagement of the supraspinatus. This was discussed earlier in the Function section.
Why a small range of motion? Because if a greater range is asked for, then neural inhibition of the upper trapezius will be overridden because the nervous system will need the upper trapezius to engage as an upward rotator to stabilize the scapula against the pull of supraspinatus (and deltoid); and if the range of motion is even greater, then the upper trapezius will engage to actually upwardly rotate the scapula, a needed motion to accompany any abduction and/or flexion motion of the humerus (due to scapulohumeral rhythm).
Once the supraspinatus engagement is felt, have the client relax and move a baby step along its course; ask the client to engage and palpate again. Continue this process until the entire belly is palpated.
What you are feeling for is the change in tissue texture when it goes from relaxation to engagement, to relaxation to engagement, i.e., soft to hard, to soft to hard.
To find the distal tendon, follow the course of the supraspinatus beyond the acromion process onto the humerus. Palpating immediately beyond the acromion, ask the client to do a gentle abduction or scaption motion and feel for the distal tendon to tauten deep to the deltoid.
Once the supraspinatus has been located, ask the client to relax and assess the health of the baseline tone of the muscle.
Role in Shoulder Impingement Syndrome
Region of impingement syndrome. Permission Dr. Joe Muscolino – The Muscular System Manual 5ed.
Shoulder impingement syndrome describes a condition in which there is impingement of soft tissues in the shoulder joint between the head of the humerus and the acromion process above. Most commonly, the distal tendon of the supraspinatus, subacromial bursa, and the long head of the biceps brachii are involved. There are many reasons why this condition occurs. One of them is that whenever the arm is abducted, if it is also not laterally rotated at the same time, then the greater tubercle jams into the acromion process, impinging the tissues located between them.
Another reason involves the inability of the scapula to upwardly rotate when the arm is abducting/flexing, which could be caused by overly facilitated scapular downward rotators (e.g., pectoralis minor) and/or overly inhibited scapular upward rotators (e.g., serratus anterior and/or upper trapezius).
Stretching the Supraspinatus
Stretching the supraspinatus. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The supraspinatus abducts and flexes the arm at the shoulder joint, therefore, bring the client’s arm into adduction with extension.
Massaging the Supraspinatus

Supraspinatus trigger points and their referral zones. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
Massaging the supraspinatus follows from knowing its palpation protocol. If the client is prone, have the client’s arm placed in some passive abduction at the shoulder joint. This will bring the scapula into upward rotation, which will slacken the upper trapezius, allowing for better access deep to it into the supraspinatus. Once you have reached the supraspinatus, it can be worked with any strokes you like. Working from proximal to distal along the supraspinous fossa works very well. When working the distal tendon, cross-fiber strokes work well to break up adhesions that might have formed.
Conclusion
The supraspinatus is an important muscle of the rotator cuff group that is often involved in shoulder impingement syndrome. But for the purpose of this blog article, it is an excellent case study for understanding how joint action terminology can lead students and therapists alike to misunderstand the function of a muscle.
Biography

Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com.
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
