Self-care for the client/patient with adductor strain (groin pull):

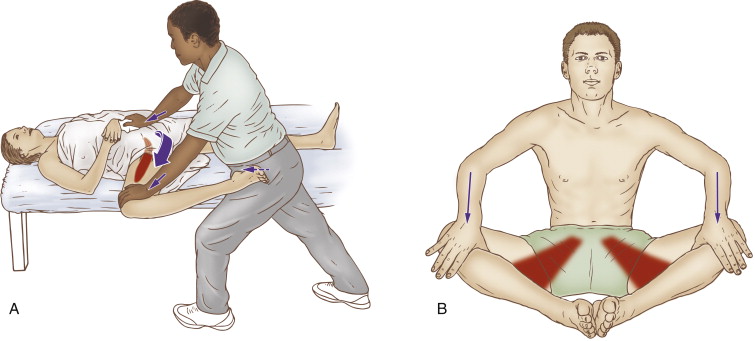
Self-care (and therapist assisted) stretch for the adductor group. Permission: Joseph E. Muscolino. The Muscle and Bone Palpation Manual, with Trigger Points, Referral Patterns, and Stretching, 2ed. (2016), Elsevier.
Self-care for the client/patient during the acute stage of an adductor strain (groin pull) is RICE: rest, ice, compression, and elevation. Of these, rest and ice are most important. Icing should be applied until the area is numb and then removed. Flexible gel ice packs are best, especially when the pack needs to contour to the client’s/patient’s body. For client/patient comfort, a paper towel or thin cloth towel should be placed between the pack and the client’s/patient’s skin.
(Note: There is considerable controversy at present about the wisdom of icing, because of the concern about the effects of diminishing the inflammation present. However, there is no doubt about the positive effects of icing to decrease pain.)
Moist heat and stretching are extremely important so that the area does not heal with excessively tight muscle tone, myofascial trigger points, and myofascial adhesions. Instruct the client/patient on how to do simple stretches into abduction. One easy method is for the client/patient to sit cross-legged and either allow gravity to stretch the thighs down into (horizontal) abduction or the client/patient can apply a very gently force with the hands on the distal thighs to increase the stretch.
During the chronic stage, appropriate rest from sports is still important, but the client/patient can recommence playing, as long as it is introduced gradually and incrementally in baby steps. It is also extremely important for the client/patient to warm up extremely well before working out. The best form of warm up involves active movements of the joints being stretched so that local circulation of fluids (blood, lymph, and synovial joint fluid) is increased, muscles are stretched and contracted, and neural patterns for movement are being grooved (facilitated). After the sporting activity is completed, then the client/patient can perform static stretching.
Medical approach to adductor strain:
The medical approach to treatment of a groin pull is usually RICE and the addition of anti-inflammatory medication, whether it is a non-steroidal anti-inflammatory drug (NSAID) or cortisone/prednisone (steroidal anti-inflammatory drug) medication. It is likely that X-Rays or an MRI might be done to rule out an internal pathologic injury. If an adductor tendon is completely or nearly completely ruptured, there is the option of surgery to sew/staple the muscle back to its attachment.
Manual therapy case study for a client with adductor strain:
Dev is a 25-year-old computer software engineer who plays soccer on weekends. Because Dev sits at a computer all day at work, he has felt increasingly stiffer over the past few years. He feels it especially when he is playing soccer. During a game about a couple of months ago, he went to kick the ball, but as he was beginning to swing his leg, an opponent blocked his kick, forcing his right thigh back into abduction and extension as he was contracting his adductor musculature to kick into the ball. He felt an immediate sharp and severe pain in his right groin and was unable to continue playing. He consulted his medical doctor on the Monday after the game who advised him to ice as often as possible and take over the counter anti-inflammatory medication, and that the condition would gradually heal. He followed the doctor’s recommendation, and about four to six weeks later, his sharp pain was gone, but he still felt mild to moderate dull pain at times and stiffness from the injury so he did not feel safe yet returning to play. For this reason, he decided to consult a clinical orthopedic massage therapist.
The therapist palpated Dev’s right thigh and found that his adductor musculature was very tight and painful. The entire adductor longus was tight and myofascial trigger points were found in other adductor muscles; and his thigh abduction range of motion was restricted. The pain was worst proximally near the pubic bone attachment of the adductor longus. Manual resistance and active range of motion into adduction and flexion of the thigh at the hip joint resulted in a mild to moderate dull pain in proximal belly/tendon of the adductor longus, near its attachment onto the pubic bone. Passive abduction of the thigh was restricted and also resulted in pain when the end of its range of motion was reached. The therapist advised Dev that although the acute phase of his adductor strain was resolved, he was still experiencing effects of the injury, primarily global tightness of the adductor longus as well as myofascial trigger points in the other adductor muscles.
For treatment, the therapist began with mild to moderate pressure soft tissue manipulation massage to the other musculature of the thigh, working around the adductors. While Dev was supine and the therapist was working the lateral and anterior musculature, a moist heating pack was placed on the adductors. The therapist then began to work directly on the adductor musculature, starting with light pressure and gradually transitioning toward deeper work. Long stripping strokes were done first, followed by cross fiber to the adductor musculature proximal tendons. The adductors were then stretched. This entire protocol was repeated a second time. The therapist then mobilized the hip joint, with special emphasis on inferior glide. With whatever time was left over, the therapist worked Dev’s other lower extremity, pelvis and low back. This protocol was performed twice a week for three weeks.
At the end of three weeks, Dev’s condition was approximately 50% better. He was no longer feeling any overt pain in the groin, and the stiff feeling each morning was moderately better. Dev continued receiving massage at a frequency of twice per week for another two weeks. He then dropped down to a frequency of once every one to two weeks. At this point in time, Dev began to play soccer again, being sure to warm up well and slowly and carefully increase the amount of playtime, so as to not to risk aggravating the condition. Dev also decided to continue seeing the massage therapist for proactive care approximately once a month.
