Altered Mechanics and Sacroiliac Joint Pain
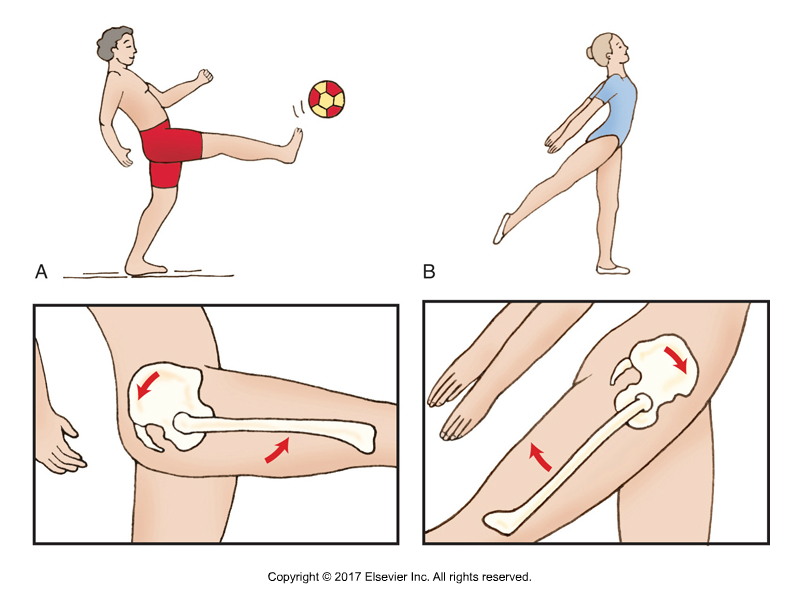
Figure A. Flexion of the thigh at the hip joint on one side while standing on support limb on the other side. Figure credit: Muscolino, Kinesiology – The Skeletal System and Muscle Function, 3rd Edition, 2017, Elsevier.
In our daily practice, we all encounter patients presenting with low back (hip / sacroiliac joint / SIJ pain), and there is no doubt that on-going low back pain results in a significant financial and economic burden to the health care system and society in general. In many instances low back pain is still poorly understood and not well managed, this is partly due to the medical profession’s dependence on costly imaging such as MRI scans and with an over-emphasis on only looking at the structure of the lumbar spine instead of evaluating the mechanics of the lumbar/ sacroiliac joints when addressing low back pain.
The spine instead should be considered as a fully integrated structure rather than only examining or treating the sensitive region. And what better place to start than at the base, in other words at the pelvis. Outside of the mainstream medical profession, there is a recognition of the importance of the pelvis and sacroiliac joints, but at the same time, there is also a lot of unnecessary confusion about how best to assess and treat the pelvis.
Lumbar Spine and Pelvis (Lumbo-Sacroiliac Region)
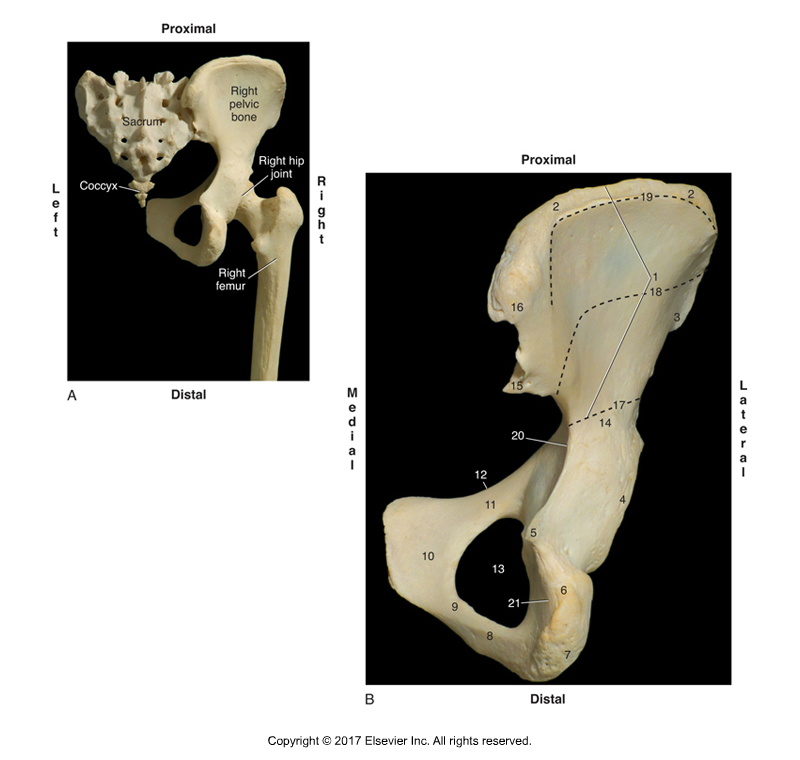
Posterior view of the right sacroiliac joint. Figure credit: Muscolino, Kinesiology – The Skeletal System and Muscle Function, 3rd Edition, 2017, Elsevier.
A primary function of the lumbar spine and sacroiliac joints of the pelvis is to transfer the loads generated by body weight and gravity during standing, walking, and sitting. During weight bearing activities, control of intra-pelvic motion (motion between the sacrum and ilium of the pelvic bone (innominate bone) is required for the transference of loads between the spine and the lower limbs. According to Panjabi (1992) stability is achieved when the passive, active, and control systems work together to produce an approximation of the joint surfaces.
The ability to effectively transfer load through the sacroiliac joints is dynamic and therefore depends on:
- Optimal function of the bones, joints, and ligaments,
- Optimal function of the muscles and fascia, and
- Appropriate neural function.
Close-Pack Position
For every joint, there is a position of maximum stability called the self-braced (close-packed) position in which there is a maximum congruence of the articular surfaces and maximum tension on major ligaments. In this position, the joint is under significant compression, and the ability to resist shear forces is enhanced by tensioning of the passive structures and increased friction between the articular surfaces. The close-pack position of the sacroiliac joint is nutation (anterior tilt rotation) of the sacrum relative to the ilium (which is relatively the same as posterior tilt rotation of the ilium relative to the sacrum).
Study
A study by Barbara Hungerford, Wendy Gilleard, Diane Lee, published in Clinical Biomechanics (2004) aimed to determine altered patterns of pelvic bone motion using skin markers in subjects with posterior pelvic (sacroiliac) pain. This study by Hungerford et al. determined whether the pattern of pelvic bone motion, determined by skin markers, differs between control subjects and subjects with sacroiliac pain.
A cross-sectional study of three-dimensional angular and translational motion of the ilium relative to the sacrum in two subject groups. Fifteen lightweight highly reflective 15 mm diameter balls were used to define the bony landmarks of each innominate, femoral segments, and the sacrum. A 6-camera motion analysis system was used to determine 3D angular and translational motion of pelvic skin markers during standing hip flexion.
Fourteen males with sacroiliac pain and healthy age and height matched against fourteen controls (with no sacroiliac pain) were studied. Each subject in the sacroiliac pain group reported unilateral pain over the posterior pelvic/SI region for greater than two months and no pain above the lumbosacral junction. The pain was consistently and predictably aggravated by activities that vertically loaded the pelvis (walking, standing, or sitting).
Tests Used

Joint play motion palpation to the sacroiliac joint. Permission Joseph E. Muscolino.
Positive results on the side of posterior pelvic pain in clinical tests for impaired lumbopelvic stabilization were looked for with the following three tests:
Active Straight Leg Raise Test: The supine patient was asked to actively flex the thigh at the hip joint while keeping the knee joint in full extension. A positive test was indicated when the pelvis failed to remain in neutral alignment, and the subject reported difficulty or inability to elevate the lower extremity.
Standing Hip Flexion Test: During a left standing hip flexion test, the subject stands on one limb and flexes the other thigh at the hip towards 90⁰. The ilium on the thigh-flexion side should posteriorly rotate relative to the sacrum, thereby dropping the PSIS (posterior superior iliac spine) relative to the sacrum. Further, the ilium on the support-limb side should also posteriorly tilt as well. A positive test was indicated when either PSIS was found to remain in a superior position relative to the sacrum, in other words, the ilium did not drop into posterior tilt.
Joint Play Motion Palpation Test: This test was used to evaluate motion of the SIJ. In this test, the ilium was challenged with manual pressure to glide relative to the sacrum.
Digital COMT
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s continuing education video streaming subscription service for massage therapists (and all manual therapists) and movement professionals, has six folders with video lessons on Manual Therapy Treatment, including an entire folder on Stretching, as well as a folder on Pathomechanics, another on Anatomy, and many more? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
Results
Active Straight Leg Raise Test: No differences were found between the pain and control groups.
Standing Hip Flexion Test: During the hip flexion component of the standing hip flexion movement, there was no significant difference in the patterning of translational motion between groups on the side of hip flexion. Posterior rotation of the ilium occurred with hip flexion in control subjects and sacroiliac pain subjects.
However, on the support-limb side, a significant difference in sacroiliac joint motion was found between subjects in the control group and subjects in the sacroiliac pain group. In the control group, posterior rotation of the weight bearing ilium occurred on the side of single leg support. However, in the sacroiliac pain group, anterior rotation occurred on the symptomatic support-limb side. In other words, on the support-limb side, the ilium rotated posteriorly in control subjects and anteriorly in symptomatic subjects.
Joint Play Motion Palpation Test: All subjects in the sacroiliac pain group demonstrated asymmetric stiffness of the SIJ when the innominate was challenged to glide relative to the sacrum, as compared to the control group.
Conclusion
Posterior rotation of the ilium, as measured using skin markers during weight bearing in controls may reflect activation of optimal lumbopelvic stabilization strategies for load transfer.
Anterior tilt rotation occurred in subjects in the pain group. Anterior tilt rotation of the ilium is not the stable close-pack position of the SIJ and this suggests a failure to stabilize intra-pelvic motion for load transfer. This is a non-optimal pattern and may indicate abnormal articular or neuromyofascial function during increased vertical loading through the pelvis. Further, joint play motion palpation of the symptomatic SIJ was found consistently in the pain group subjects.
Comment by Joseph E. Muscolino
Both of these study’s findings support the concept that altered mechanics of the SIJ are correlated with the presence of SIJ pain. This points to the value that all manual and movement therapies can have toward alleviating sacroiliac joint pain in clients and patients that present to us. Massage therapy, stretching, joint mobilization (slow oscillation Grade IV or fast thrust Grade V) would all be of value, as well as Pilates, yoga, and fitness strength training for stability. Therefore, depending on the mechanics that are underlying the client’s SIJ condition, manual therapists and movement professionals may be ideally suited to help clients who present with sacroiliac pain.
This blog post article was created in collaboration with www.terrarosa.com.au.
Did you know that Digital COMT (Digital Clinical Orthopedic Manual Therapy), Dr. Joe Muscolino’s continuing education video streaming subscription service for massage therapists (and all manual therapists) and movement professionals, has six folders with video lessons on Manual Therapy Treatment, including an entire folder on Stretching, as well as a folder on Pathomechanics, another on Anatomy, and many more? Digital COMT adds seven new video lessons each and every week. And nothing ever goes away! Click here for more information.
