Rotator Cuff Pathology – Introduction:
Rotator cuff pathology involves the rotator cuff muscles at the glenohumeral joint. Permission: Joseph E. Muscolino, The Muscle and Bone Palpation Manual with Trigger Points, Referral Patterns, and Stretching, 2ed. (2016), Elsevier.
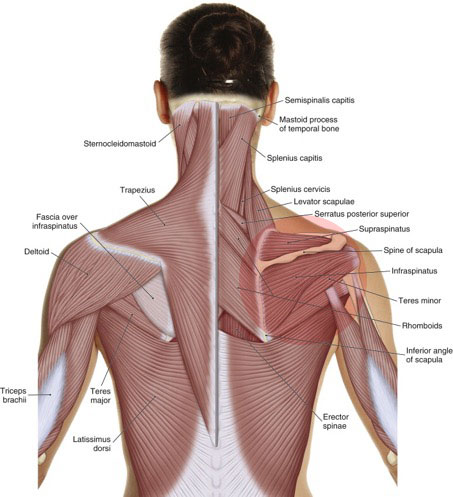
The four rotator cuff muscles are the supraspinatus, infraspinatus, teres minor, and the subscapularis. The two most common types of rotator cuff pathology are rotator cuff tendinitis and rotator cuff tear. Excessive physical stress placed on the rotator cuff tendon can cause irritation and inflammation, in other words, tendinitis. If the physical stress is chronic and/or excessive, degeneration or a tear in the rotator cuff tendon might occur (tendinosus). A tear can be partial or a complete rupture. It should be noted that chronic tendinitis can lead to degeneration of the rotator cuff tendon collagen structure. When this occurs, the principal problem is no longer inflammation; it is degeneration, which has implications for treatment. Further, degeneration increases the likelihood that the tendon will tear.
As a general rule, rotator cuff tendinitis is less severe than a rotator cuff tear, and degeneration is midway between the two.
Causes:
Each of the rotator cuff muscles has its own concentric glenohumeral (GH; shoulder) joint action for motion: the supraspinatus abducts and flexes; the infraspinatus and teres minor laterally rotate; and the subscapularis medially rotates. However, as a group the rotator cuff muscles are primarily important for isometric stabilization at the GH joint. Whenever the distal end of the humerus is moved upward, which occurs with flexion, extension, abduction, and adduction from anatomic position, the head of the humerus must be stabilized down into the glenoid fossa of the scapula. The rotator cuff muscles are primarily responsible for this stabilization. Because they engage for motion and also for stabilization, they are often overused and injured. This is especially true for someone whose job involves continual use of the shoulder joint, such as an assembly line worker or a carpenter. Overuse injury is also common in athletes, such as baseball and tennis players. Overhead postures and movements of the arm are especially problematic because they increase the likelihood of impingement of the rotator cuff tendon (usually the supraspinatus tendon). Besides chronic microtrauma overuse, rotator cuff pathology can also occur due to a macrotraumatic injury such as a fall or a motor vehicle accident.
The most commonly injured part of the rotator cuff tendon is the supraspinatus distal tendon where it travels between the acromion process and the head of the humerus. Whenever the arm is lifted into abduction, the supraspinatus tendon can become impinged. This is prevalent in clients who repeatedly or chronically have their arms raised to the side. Examples are baseball pitchers, barbers/hair stylists, and a person who sleeps with their arm(s) above their head.
Impingement of the supraspinatus between the head of the humerus and the acromion process of the scapula is also more common if the scapulohumeral kinematic motions of the humerus and scapula are not healthy. For example, if the arm is medially (internally) rotated as it is abducted, the greater tubercle of the humerus will hit the acromion process, pinching the supraspinatus tendon between them; this problem is especially prevalent for clients with upper crossed syndrome “rounded shoulders.” If the arm is laterally (externally) rotated instead, the smaller lesser tubercle will align with the acromion, affording more room and therefore less chance of impingement. For this reason, it is extremely important to make sure that the arm is laterally rotated whenever it is lifted to the side.
It is also important for the scapula to upwardly rotate during arm abduction because this affords more room for the head of the humerus when the arm is raised, thereby decreasing the likelihood of tendon impingement. If the scapular upward rotator muscles (upper and lower trapezius and serratus anterior) are weak/inhibited and/or the downward rotator muscles (pectoralis minor, levator scapulae, rhomboids) are tight/overly facilitated, scapular upward rotation might be limited, causing impingement of the supraspinatus tendon.
Another factor that can contribute to pathologic changes in the supraspinatus tendon is decreased arterial blood flow. This can occur when the tendon is impinged as described earlier, but it can also occur when the arm is hanging because the tension force of the weight of the arm can pull the arteries taut and diminish their interior lumen size, which decreases their ability to carry blood to the rotator cuff tissue. As with impingement, this happens most often with the supraspinatus tendon. Because the supraspinatus tendon is the most often injured part of the rotator cuff, it is called the critical zone of the rotator cuff tendon.

