Note: This blog post article is the tenth in a series of twelve articles on musculoskeletal conditions of the low back (lumbar spine) and pelvis. For the rest of the articles in the series, scroll to the end of this article.
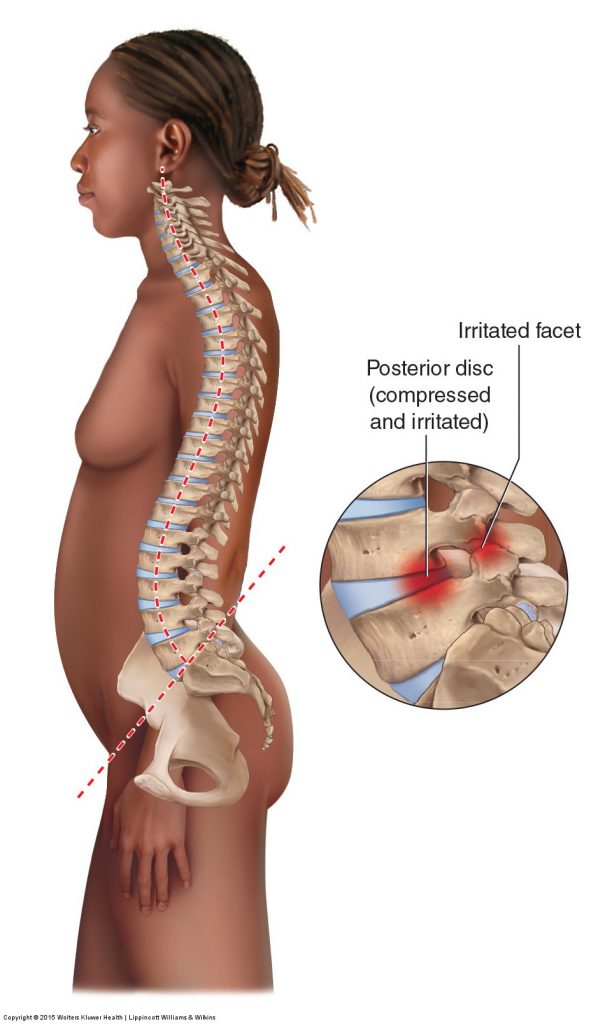
Figure 22. A hyperlordotic lumbar spine of lower crossed syndrome places greater weight-bearing force on the facet joints and the posterior discs. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015.
The lumbosacral spine should have a healthy degree of both anterior pelvic tilt and lumbar lordosis. If the anterior tilt is excessive, the lumbar lordotic curve will also be excessive, and the client will have a postural distortion pattern known as lower crossed syndrome.
Description of Anterior Pelvic Tilt and Hyperlordotic Lumbar Spine
When the lumbar lordosis is excessive, it is described as a hyperlordotic lumbar spine (hyperlordosis), and commonly called a swayback. The problem with this condition is that it places excessive pressure on the facet joints of the spine and the posterior margins of the discs (Fig. 22). This can lead to irritation, injury, and pain. This can be easily felt by simply tilting the pelvis anteriorly and arching the back; this usually causes immediate low back discomfort or pain. More seriously, because lumbar extension/lordosis decreases the size of the intervertebral foramina as well as the central spinal canal, this condition can predispose the client to nerve compression. Increased compression to the facets and posterior disc margins can also further the progression of degenerative joint disease (osteoarthritis), causing increased bone spurs, which can also further aggravate nerve compression.
Note: The Terms Lordosis and Lordotic
Because many people use the terms lordosis and lordotic to denote an excessive and unhealthy lordotic curve/lordosis, it is important to understand whether a person is referencing to a normal lordosis or an excessive lordosis when using these terms. An excessive lordosis is most accurately termed a hyperlordosis/hyperlordotic curve.
Mechanism and Causes of Lower Crossed Syndrome
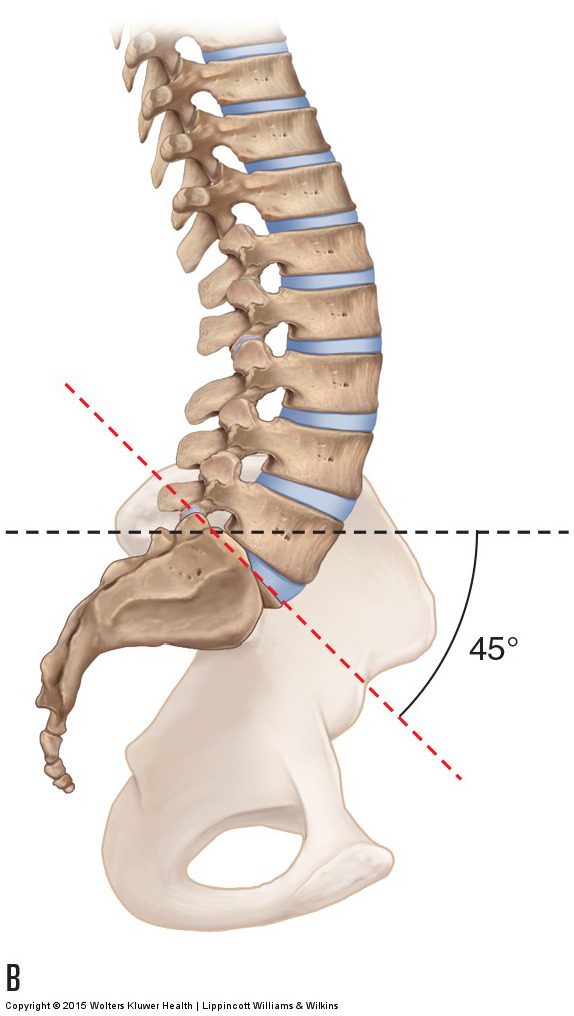
The cause of lower crossed syndrome, in other words excessive anterior pelvic tilt and hyperlordotic lumbar spine is almost always the increased anterior tilt posture of the pelvis. The lumbar spine sits on the sacrum of the pelvis. If the sacrum tilts anteriorly within the sagittal plane, the lumbar spine must compensate by increasing its extension/lordosis to maintain the head upright so that you can see forward and have your ears level for balance. The degree of a person’s pelvic tilt is measured by the sacral base angle. The sacral base angle is formed by drawing two lines, one horizontal and another along the base of the sacrum, and then measuring the angle formed between them. A sacral base angle of approximately 30 degrees is usually stated as being ideal. A greater sacral base angle results in a hyperlordotic lumbar spine, and a lesser sacral base angle results in a hypolordotic lumbar spine (Fig. 23). Therefore, the root of a lumbar hyperlordosis usually rests in the sagittal plane posture of the pelvis. Treatment must be directed toward remedying the increased anterior pelvic tilt. Excessive anterior tilt can also be caused or increased by excessive weight carried anteriorly in the abdominal region. Further, if an excessive pelvic anterior tilt and lumbar hyperlordotic posture become chronic, ligament laxity/tautness will occur as well as fascial adhesions that resist normalization of this condition.
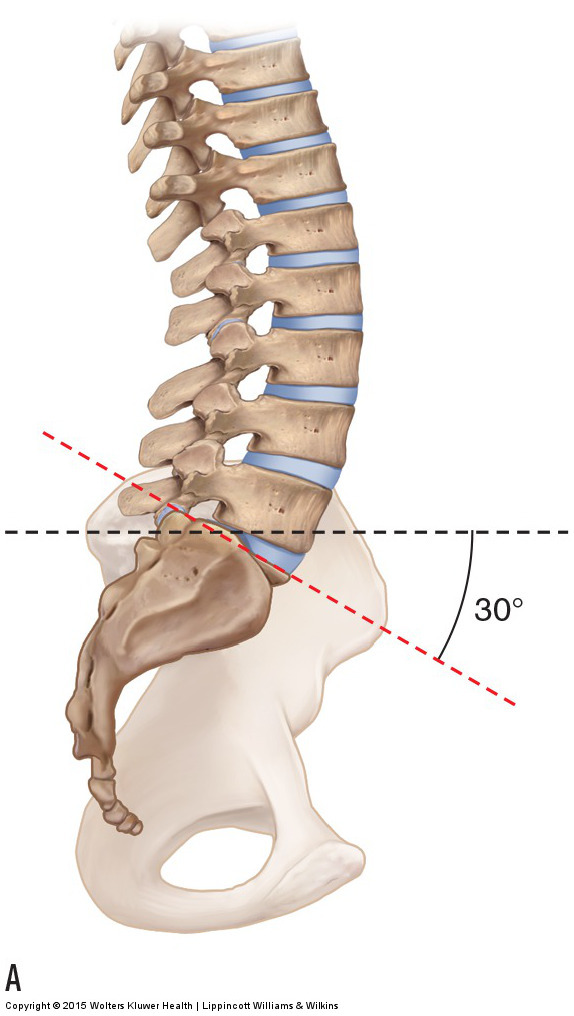
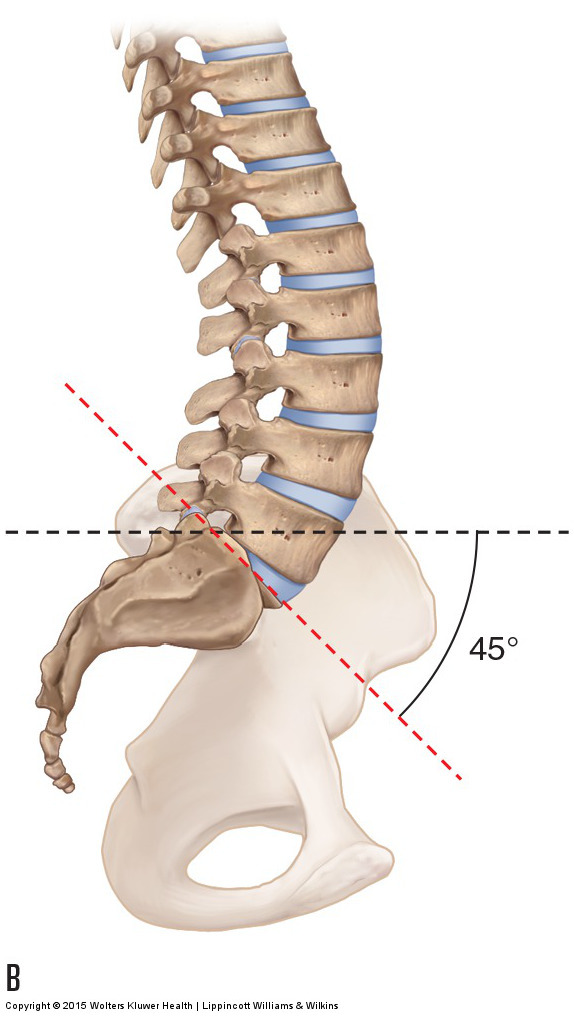
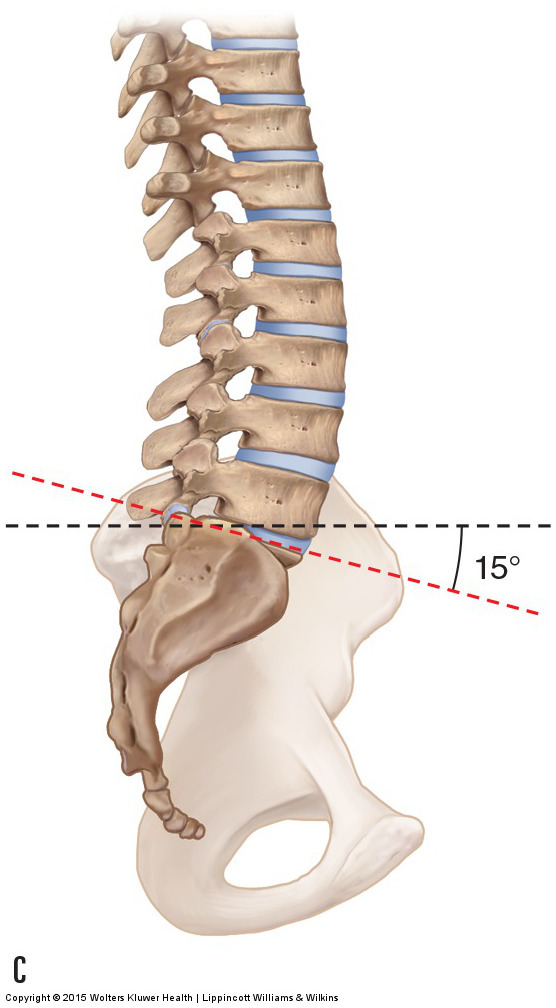
Figure 23. Lower Crossed Syndrome: sacral base angle and lumbar lordosis. The sacral base angle is formed by measuring the intersection of a line drawn along the base of the sacrum and a horizontal line. (A) Normal sacral base angle of 30 degrees and a healthy lumbar lordosis. (B) An increased sacral base angle results in increased lumbar lordosis. (C) A decreased sacral base angle results in decreased lumbar lordosis. Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015.
Muscles of Pelvic Tilt
The tilt posture of the pelvis in the sagittal plane that is responsible for lower crossed syndrome is determined by the forces placed on it. Most commonly, these forces result from muscle pulls. Within the sagittal plane, the hip flexor muscle group and the low back extensor muscle group do anterior tilt of the pelvis, and the hip extensor muscle group (gluteals and hamstrings) and the anterior abdominal wall muscle group do posterior tilt of the pelvis. It is very common for hip flexor and low back extensor anterior tilters to be excessively tight and for the anterior abdominal wall and gluteal region posterior tilters to be excessively weak. It is often stated that the anterior tilters are facilitated and the posterior tilters are inhibited in tone. When viewing this pattern from the side, you see that a cross (“X”) is formed, with one arm of the cross representing the facilitated anterior tilters and the other arm representing the inhibited posterior tilters. Because of this crossed pattern, this condition is often described as the lower crossed syndrome (there is an upper crossed syndrome in the upper body as well) (Fig. 24). This term was coined by a Czech physiologist named Vladimir Janda.
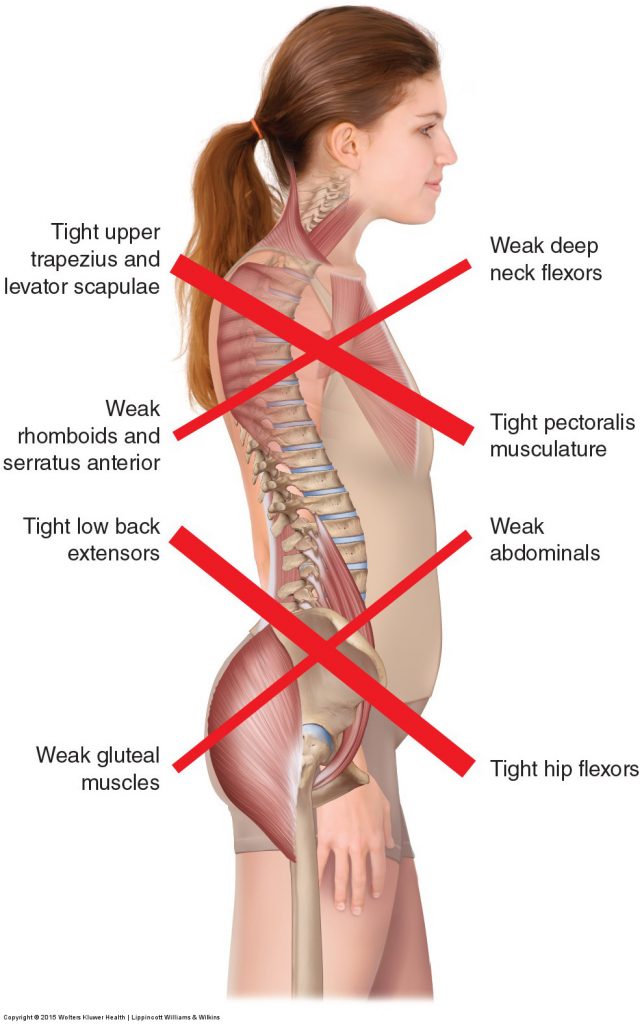
Figure 24. Lower crossed syndrome (and upper crossed syndrome). Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach. 2015.
Note: Pelvic Posture and “Swayback”
The term swayback can be used to describe two different postural distortion patterns of the lumbosacral region. It can be used to describe the lower crossed pattern of excessive anterior tilt of the pelvis and hyperlordosis of the lumbar spine (because the lumbar spine “sways back”). However, it is also used to describe an excessive posterior tilt of the pelvis (because the pelvis “sways back”), which is usually accompanied by a hypolordotic lumbar curve. For this reason, the term swayback is ambiguous and when used should be clearly defined.
Note: Treatment Considerations in Brief for Anterior Pelvic Tilt and Hyperlordotic Lumbar Spine
Soft tissue work for clients with increased anterior tilt of the pelvis and the compensatory hyperlordosis of the lumbar spine that follows is extremely valuable. The primary goal for the manual therapist is to loosen anterior tilters of the pelvis (hip flexors and low back extensors) and to have the client strengthen posterior tilters of the pelvis (anterior abdominal wall and gluteal muscles in the buttocks).
This blog post article is the tenth in a series of twelve articles on musculoskeletal conditions of the low back (lumbar spine) and pelvis.
The articles in this series are:
- Hypertonic / tight muscles
- Myofascial trigger points
- Joint dysfunction
- Sprains and strains
- Sacroiliac joint injury
- Pathologic disc conditions and sciatica
- Piriformis syndrome
- Degenerative joint disease (DJD)
- Scoliosis
- Lower crossed syndrome
- Facet syndrome
- Spondylolisthesis
