Introduction
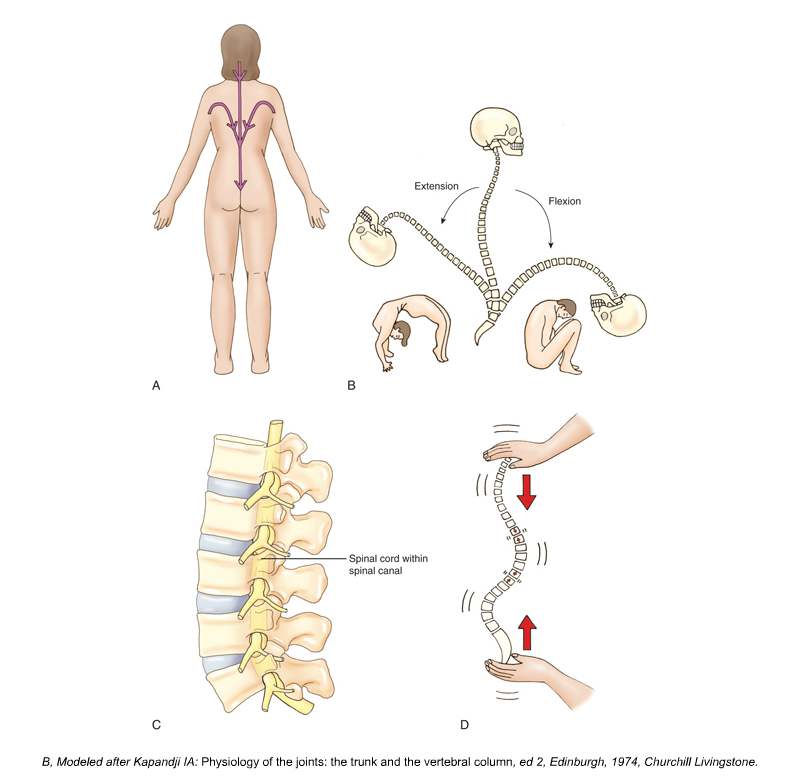
Figure 1. Sagittal plane motion of the spine (See Figure b). Permission Joseph E. Muscolino. Kinesiology: The Skeletal System and Muscle Function, 3rd Ed. Elsevier. Modeled from Kapandji, IA, Physiology of the Joints: The Trunk and the Vertebral Column, 3rd Ed. Elsevier.
The spine is an incredible structure. It exhibits both tremendous stability and mobility. It must be stable enough to provide the structural support for the axial body and yet also be flexible enough to allow for movement in all three cardinal planes. Indeed, the spine allows for 255 degrees of motion in the sagittal plane, 180 degrees of motion in the frontal plane, and 240 degrees of motion in the transverse plane (Figure 1). This is no easy feat because greater mobility usually comes at the expense of lesser stability; and greater stability usually means lesser mobility. The spine is able to successfully accomplish both ends of the spectrum. Much of the key to the spine’s capacity for stability and flexibility lies in the structure of its curves.
Curves of the Spine
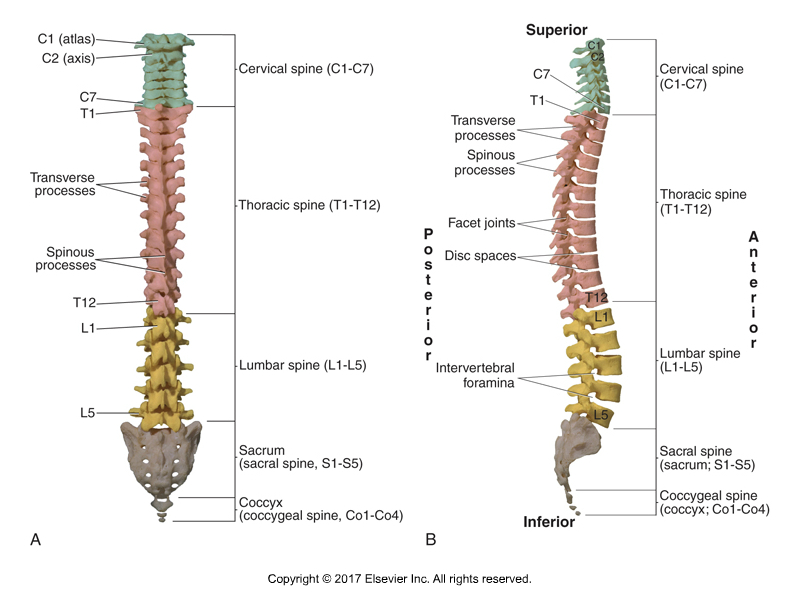
Figure 2. A, Posterior view of the straight spine. B, Lateral view of the four sagittal plane curves of the spine. Permission Joseph E. Muscolino. Kinesiology: The Skeletal System and Muscle Function, 3rd Ed. Elsevier.
In the frontal and transverse planes, the adult spine should ideally be straight and have no curves (Figure 2A). However, the adult spine has four sagittal plane curves: two primary kyphotic curves in the thoracic and sacrococcygeal regions, and two secondary lordotic curves in the cervical and lumbar regions (Figure 2B).
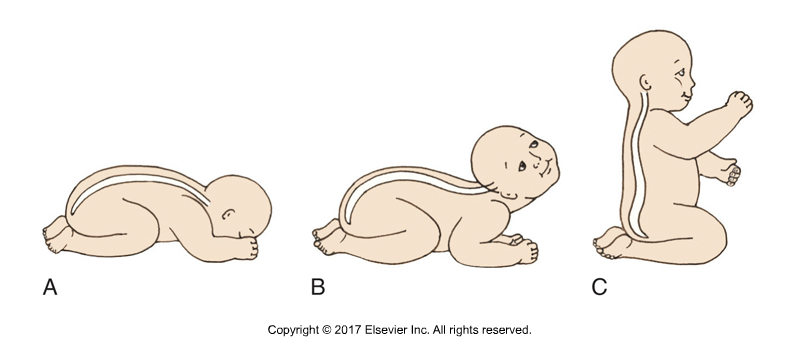
Figure 3. Kyphotic and lordotic curves of the spine. A, At birth. B, The cervical lordosis forms when we raise out head. C, The lumbar lordosis forms when we sit up. Permission Joseph E. Muscolino. Kinesiology: The Skeletal System and Muscle Function, 3rd Ed. Elsevier.
A kyphotic curve, by definition, is a curve of flexion and has its convexity posterior and its concavity anterior, whereas a lordotic curve is a curve of extension and has its convexity anterior and its concavity posterior. The kyphotic curves are described as primary because they form first. In fact, when we are born, our entire spine is one large kyphotic curve. Lordotic curves form later; hence they are described as secondary. The cervical lordosis forms when an infant lifts its head to see the world; and the lumbar lordosis forms when the infant learns to sit up (Figure 3).
Note: Sagittal Plane Curve Terms
There is a great deal of confusion regarding the terms used to describe the sagittal plane curves of the spine. A kyphotic curve is a kyphosis (plural: kyphoses); and a lordotic curve is a lordosis (plural: lordoses). The terms kyphosis and lordosis are often misused in that they are used to describe an individual who has an excessive kyphotic or lordotic curve. It is normal and healthy to have a kyphosis in the thoracic and sacrococcygeal regions and to have a lordosis in the cervical and lumbar regions. An excessive kyphosis should correctly be termed a hyperkyphosis or a hyperkyphotic curve; and excessive lordosis should correctly be termed a hyperlordosis or a hyperlordotic curve. Similarly, a decreased curve would be termed a hypokyphosis or hypokyphotic curve, and a hypolordosis or hypolordotic curve.
Altered Spinal Curves:
Maintaining healthy spinal curves is extremely important. Any postural deviation from ideal structure may potentially cause dysfunction and/or pain. Altered curve structure can occur in all three cardinal planes.
Sagittal Plane
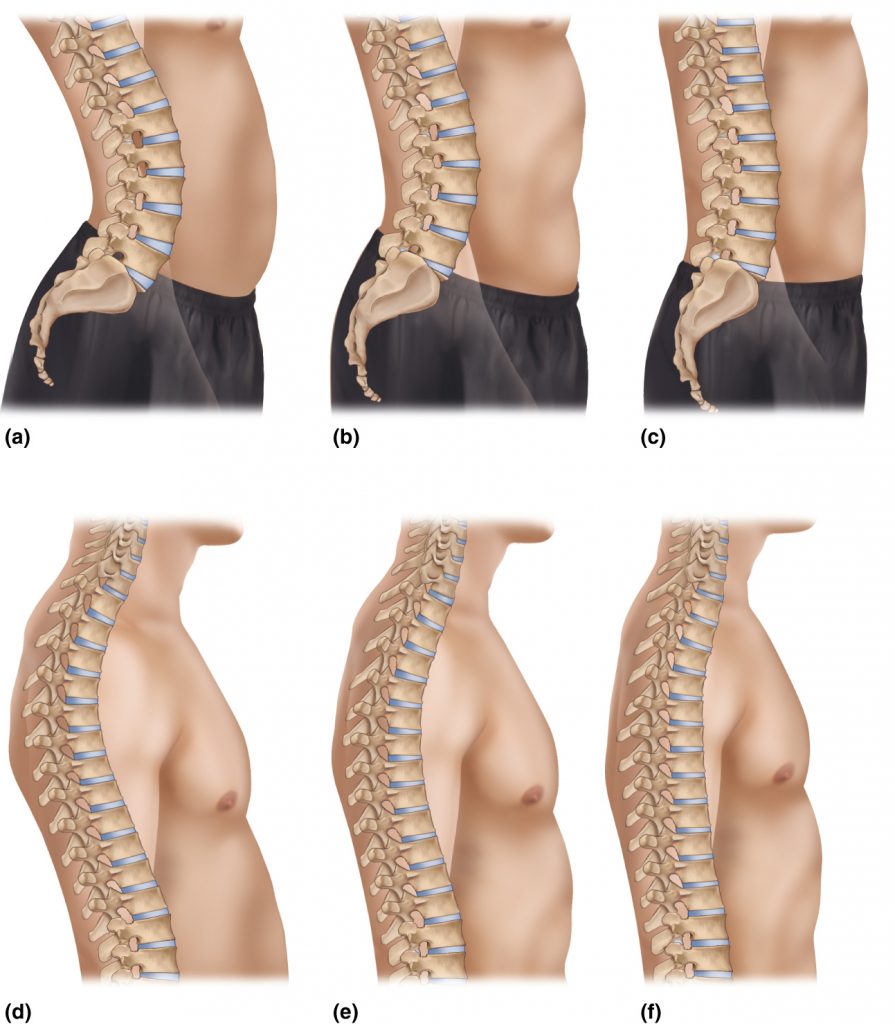
Figure 4. A, Hyperlordotic lumbar spine. B, Healthy lumbar spine. C, Hypolordotic lumbar spine. D, Hyperkyphotic thoracic spine. E, Healthy thoracic spine. F, Hypokyphotic thoracic spine. Permission Joseph E. Muscolino.
Dysfunctional postures in the sagittal plane are hyperlordotic, hyperkyphotic, hypolordotic, and hypokyphotic curves. As their names imply, hyperlordoses and hyperkyphoses are excessive lordotic and kyphotic curves respectively, and hypolordoses and hypokyphoses are decreased lordotic and kyphotic curves respectively (Figure 4). Both hyperlordotic and hypolordotic lumbar spines are common postural deviation patterns. The thoracic spine is more often hyperkyphotic than hypokyphotic, but both postural deviation patterns do occur. Note: The cervical spine is interesting in that the lower cervical spine is usually hypolordotic, but the upper cervical spine is usually hyperlordotic as a compensation to bring the head back to level. Because the sacrum is a fixed bone, it is not susceptible to postural deviation patterns.
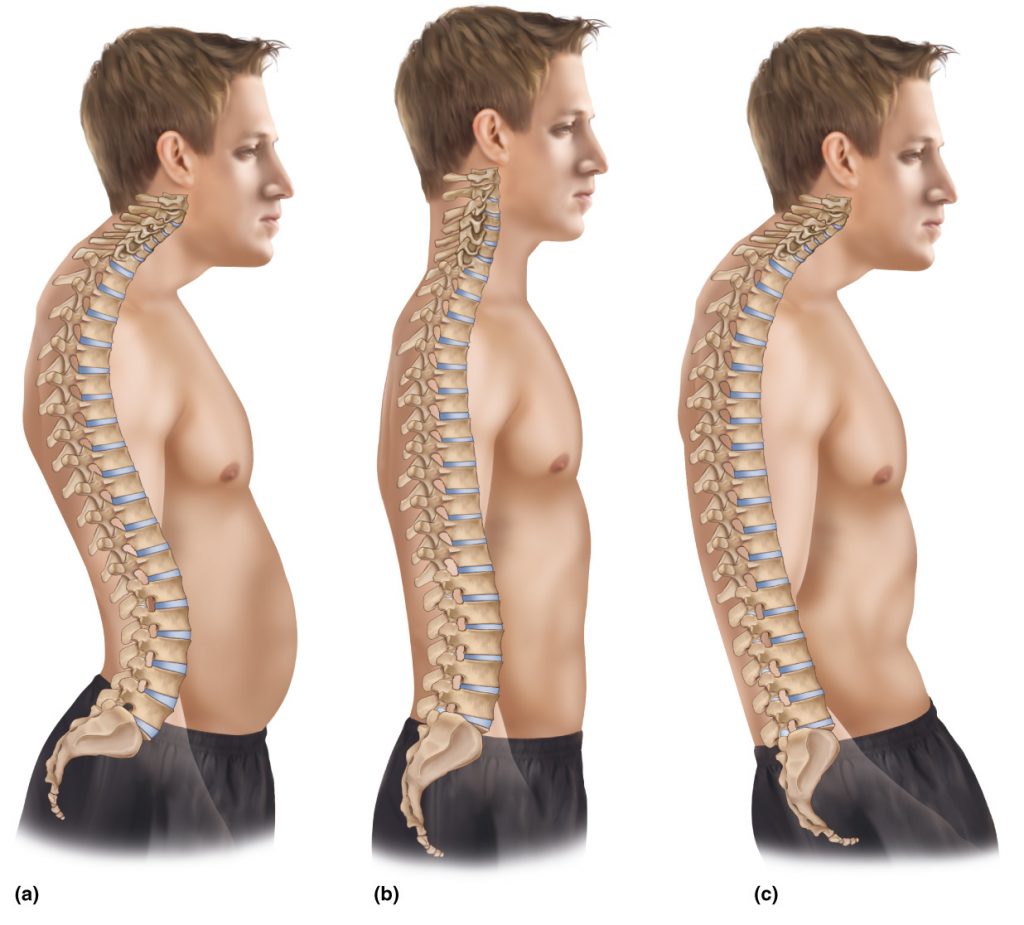
Figure 5. Three common sagittal plane postural deviation patterns in the spine. A, Hyperlordotic lumbar spine, hyperkyphotic thoracic spine, hypolordotic lower cervical spine, and hyperlordotic upper cervical spine. B, Hypolordotic lumbar spine, hypokyphotic thoracic spine, hypolordotic cervical spine. C, Kyphotic lumbar spine, hyperkyphotic thoracic spine, hypolordotic lower cervical spine, and hyperlordotic upper cervical spine. Permission Joseph E Muscolino
Given that the multiple regions of the spine comprise one column, it makes sense that a postural deviation pattern in one region of the spine will usually result in a compensatory postural deviation pattern in the adjacent region. For example, it is common for a hyperlordotic lumbar spine to cause a compensatory hyperkyphotic thoracic spine, which in turn, results in a hypolordotic lower cervical spine and compensatory hyperlordotic upper cervical spine (Figure 5A). Similarly, a hypolordotic lumbar spine often results in a hypokyphotic thoracic spine, with a hypolordotic cervical spine (Figure 5B). Interestingly, a reverse lumbar curve, in other words a kyphotic lumbar spine, usually results in the same compensatory pattern as the hyperlordotic lumbar spine: a hyperkyphotic thoracic spine, a hypolordotic lower cervical spine, and a hyperlordotic upper cervical spine (Figure 5C). It should be noted that sagittal plane postural distortion of the lumbar spine is most often due to altered anterior/posterior tilt posture of the pelvis, as can be seen in Figures 5A, B, and C.
Note: Treating the Cause
Permission Joseph E. Muscolino
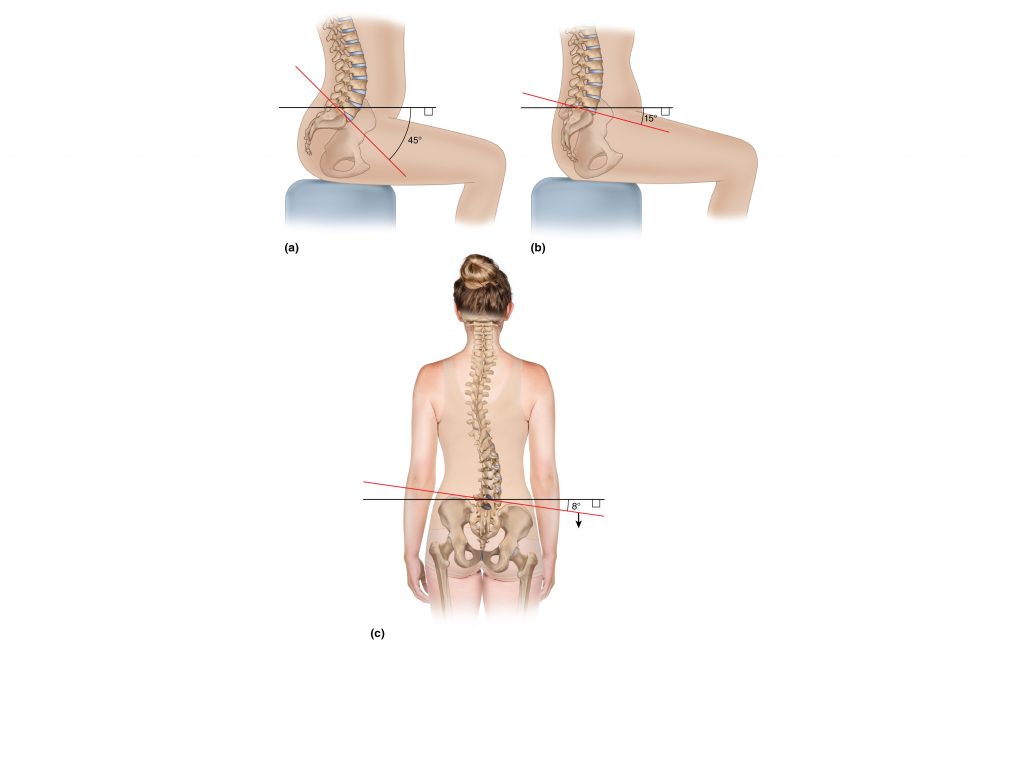
When a client presents with spinal curve dysfunctional posture, it is imperative to directly address the altered spinal posture with stretching and strengthening. However, it is also imperative to determine the underlying cause of the condition and address that as well. Altered spinal posture often follows from altered posture of the pelvis. For example, in the sagittal plane, an increased anterior pelvic tilt results in lumbar hyperlordosis (Figure A), and a decreased pelvic tilt results in lumbar hypolordosis (Figure B). And in the frontal plane, a laterally tilted (depressed) pelvis results in a scoliosis with the convexity on the side to which the pelvis is laterally tilted/depressed (Figure C). If a pelvic obliquity is found, then it is important to determine its cause. Perhaps it is due to an imbalance of musculature that acts on the pelvis. For example, overly tight/facilitated hip joint flexors and/or weak/inhibited hip joint extensors would result in an excessive anterior tilt of the pelvis. Or an overly tight/facilitated quadratus lumborum can elevate the pelvis on one side, altering its frontal plane posture. Or perhaps the underlying cause starts at the very foundation of the body at the feet: An overly pronated foot that results in a collapsed arch would likely cause the pelvis to laterally tilt to that side.
Frontal and Transverse Planes

Figure 6. A scoliosis is defined as a frontal plane lateral flexion deviation of the spine. Because lateral flexion couples with rotation, a scoliotic curve also involves transverse plane rotation.Permission Joseph E, Muscolino
Because the spine is supposed to be straight within the frontal plane, any frontal plane curve is technically a postural distortion pattern and defined as a scoliosis. And because the facet joints of the spine do not allow pure frontal plane motion, transverse plane motion couples with frontal plane motion. For this reason, a scoliotic curve also involves transverse plane rotation in addition to the frontal plane lateral flexion (Figure 6).
Stretching and Strengthening Altered Spinal Curves
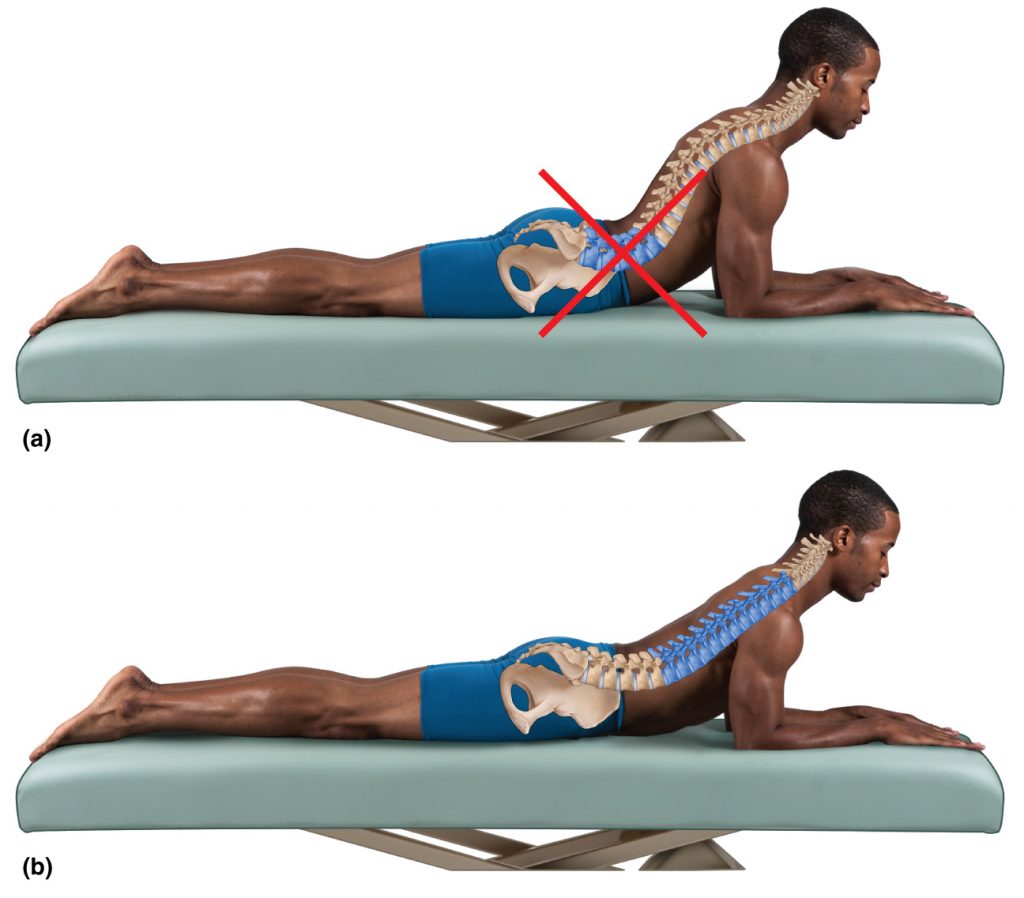
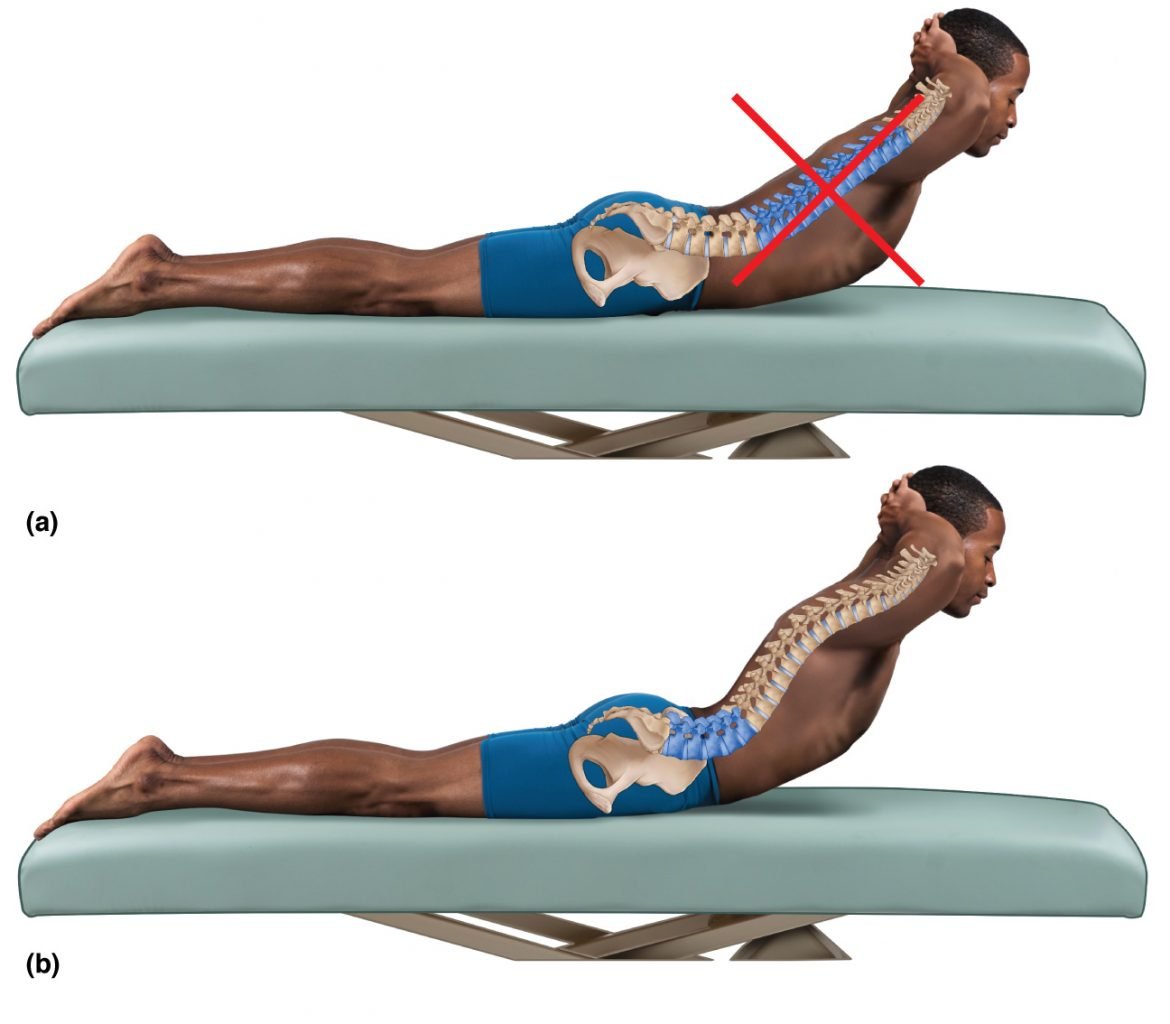
Figure 7. A, Spinal stretch into extension with the motion occurring at the lumbar spine. B, The same exercise with the extension motion focused on the thoracic spine. Permission Joseph E. Muscolino
Bones are passive elements that are positioned posturally or are moved dynamically based on the forces that act upon them. These forces may be external to our body, the most common example being gravity; or they may be internal to our body, usually due to active tension forces of muscle contraction and passive tension forces from fascial tissues. It is important to assess and treat postural dysfunctional spinal curves because if not addressed, they will likely become entrenched and worsen in time, due to both the creation of fascial adhesions and the tightening of associated musculature. Although spinal postural distortion patterns are often symptom-free in the short run, when left untreated, in the long run, they inevitably lead to decreased mobility, and often pain.
Manual therapy can be extremely effective when working with a client with spinal postural distortion. However, due to the stubborn nature of this condition, the inclusion of client self-care stretching and strengthening in the treatment strategy is of paramount importance. However, the manner in which the stretching and strengthening is done is extremely important. It is not enough to simply recommend that the client move in one direction or another. The key is to focus the effect of the exercise to the correct region of the spine.
For example, if the client’s thoracic spine is hyperkyphotic (in other words, excessively flexed), it makes sense to recommend self-care spinal extension stretching to the client with the hope of decreasing the thoracic hyperkyphosis. However, if the client is not taught to focus the extension stretch on the thoracic region, it is likely that the lumbar spine will move instead because its natural curve, lordosis, is a curve of extension (Figure 7A). As a result, if the thoracic spine is never required to extend, in time it will become hypomobile with regard to extension and locked into flexion. In effect, the hypomobility (decreased extension) of the thoracic spine is compensated for by a relative hypermobility (increased extension) of the lumbar spine. Similarly, if the lumbar spine continually compensates for the thoracic spine’s lack of extension, the lumbar spine will become hypermobile into extension, and likely become hyperlordotic.
Therefore, simply directing the client to perform spinal extension may not only be ineffective at improving the thoracic hyperkyphosis, but also may serve to cause or increase lumbar hyperlordosis. For this reason, the client needs to be educated how to properly perform the spinal extension stretch so that its effect is focused on the thoracic spine and not the lumbar spine (Figure 7B). One effective way to help the client feel where they need to stretch is to physically cue the client by gently touching the region of the spine where the stretch should occur. This can help to increase their proprioceptive awareness when performing the stretch.
Following are proper sagittal plane and frontal plane stretching and strengthening exercises for altered postural curves of the lumbar and thoracic regions of the spine.
Note: Stretching and Strengthening Protocols
There are many types of stretching protocols that can be recommended to the client. Two excellent stretching methods that are easy for a client to perform are static and dynamic stretching. Static stretching is performed by asking the client to attain a position of stretch and then hold it statically for a prolonged period of time. A good guideline is to perform three repetitions, each one held for approximately 20 seconds (this results in a stretch time of one minute). Dynamic stretching, as its name implies, is more motion oriented. Instruct the client to hold the position of stretch for only two to three seconds, but to perform more repetitions, perhaps as many as 20 (again totaling one minute for the stretch). Another approach is to perform a hybrid of static and dynamic stretching. Instruct the client to perform approximately 40 seconds of dynamic repetitions and then finish with one long 20-second static stretch repetition (again totaling one minute for the stretch). Note that whether the stretch is performed statically, dynamically, or a hybrid of the two, a good guideline is to recommend that the client spend approximately one minute on each stretch.
Strengthening exercise protocols can also vary. As with stretching, there is a choice of holding the position attained for a short period of time and performing many repetitions, or holding the position of the exercise for a longer period of time with an isometric contraction, but performing only a few repetitions. Either way, a good target for the client to work toward is to perform the exercise for a total of one minute.
It is important to note that any exercise, whether it is a stretching or strengthening exercise, acts as a stressor that challenges the body to change. If performed properly, the body becomes healthier. However, if performed too aggressively, it can injure the body. When recommending self-care for the client, it is extremely important to emphasize that the client needs to gradually build up the time and intensity of the exercise. It may take a little longer to reach the desired goal, but the client will be assured of reaching it without injury.
Sagittal Plane Stretching and Strengthening
Thoracic Hyperkyphosis
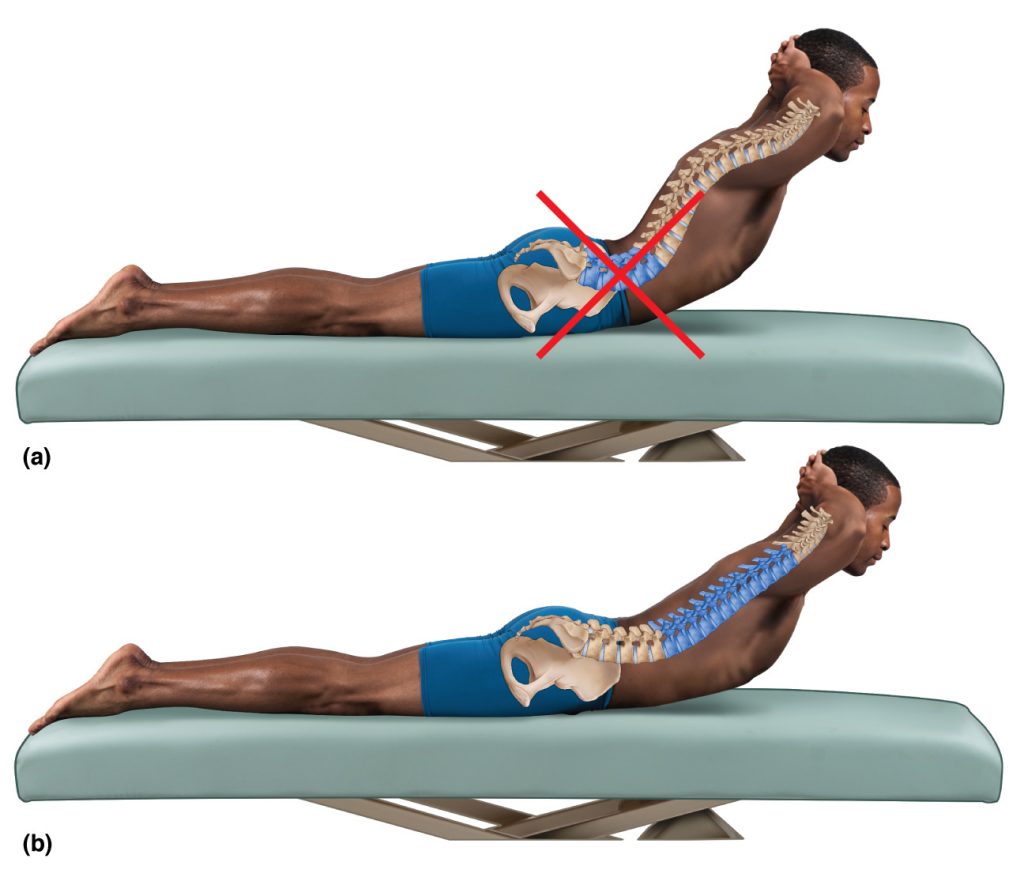
Figure 8. A, Extension strengthening exercise performed from the lumbar spine. B, Extension strengthening exercise performed from the thoracic spine.
Figure 7 demonstrated how to perform stretching for an excessive thoracic kyphotic curve. Strengthening a hyperkyphotic thoracic spine is performed in a similar manner. The difference is that instead of simply placing the spine in a passive position of thoracic extension, it is necessary to engage spinal extension musculature to attain and hold this position. What is most important is that the client moves from the thoracic region and not the lumbar region (Figure 8).
Lumbar Hyperlordosis
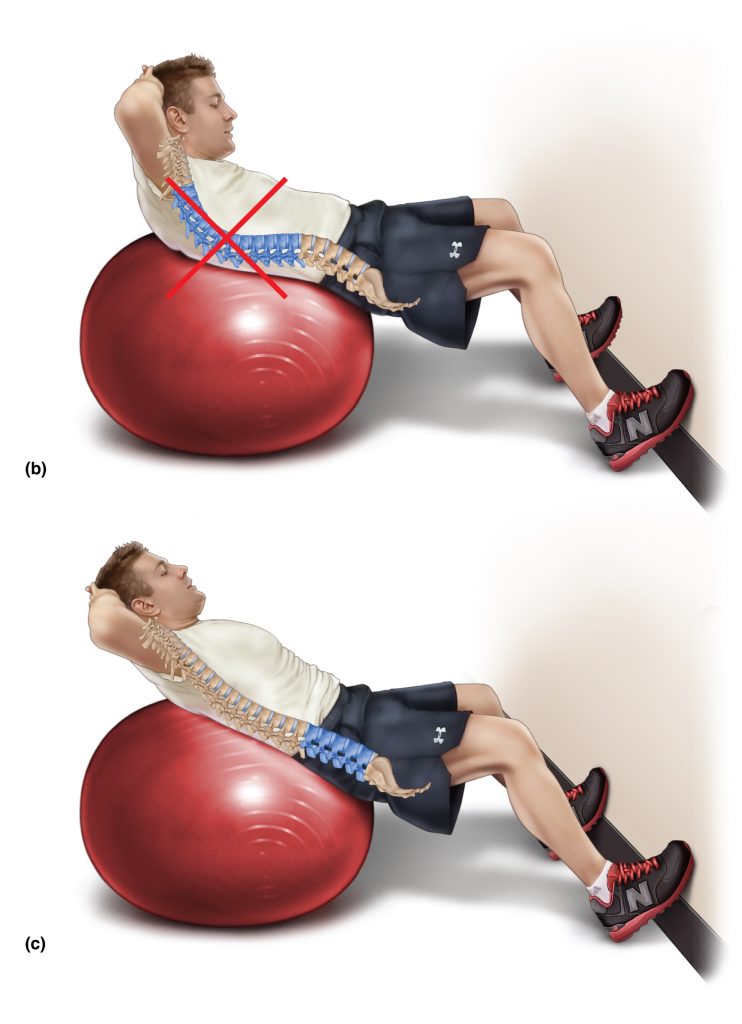
Figure 9. Flexion exercises for the spine. A, Passive stretch of the lumbar spine. B and C, A gym ball is used to perform flexion strengthening exercise for the spine. B, The client initiates the motion from the thoracic spine. C, The client initiates the motion from the lumbar spine, which can help to mobilize and reverse a lumbar hyperlordosis. (Figure A Permission Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis: A Clinical Orthopedic Approach. (2015)

Permission Joseph E. Muscolino
If a client has a hyperlordotic lumbar spine, then because a lordotic curve is a curve of extension, it is important for the client to move into flexion and to create this motion at the lumbar spine. Figure 9A demonstrates (therapist-assisted) double knee to chest stretch, which is an effective passive stretch into flexion to reverse a hyperlordotic lumbar spine. Figures 9B and C demonstrate flexion strengthening exercises for the spine. The focus needs to be on initiating the motion from the lumbar spine and not the thoracic spine. If a typical “curl-up” exercise is performed in which the client only curls up (flexes) approximately thirty degrees (Figure 9B), then it is likely that the motion will occur only in the thoracic region and will not be as effective toward reducing the lumbar hyperlordosis. Instead, the client needs to focus on effecting the movement from the lumbar spine while keeping the thoracic spine either in extension or in neutral position (Figure 9C).
Thoracic Hypokyphosis
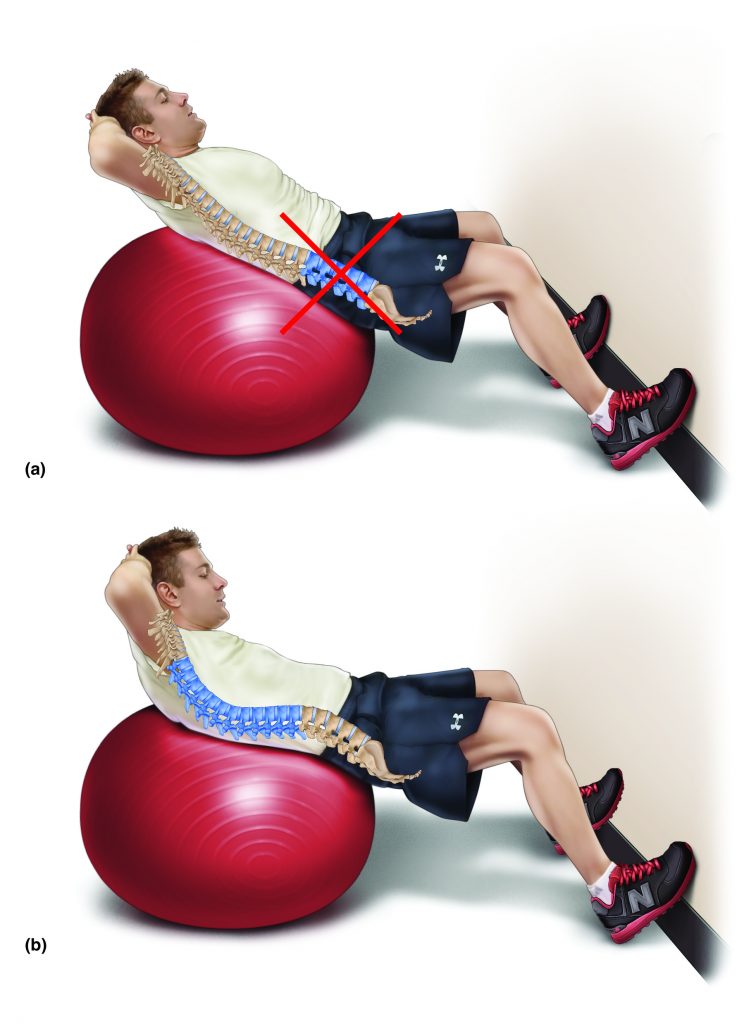
Figure 10. Curl-up flexion exercise for a hypokyphotic thoracic spine. The motion should not be occurring at the lumbar spine (A). Rather it should be created in the thoracic spine (B). Permission Joseph E. Muscolino.
If the client has a hypokyphotic thoracic spine, then the directions are essentially opposite to what was recommended for the client with a lumbar hyperlordosis. Now the client should be instructed to perform a curl-up spinal flexion exercise to only approximately thirty degrees so that the motion is focused on the thoracic spine and not the lumbar spine (Figure 10).
Lumbar Hypolordosis
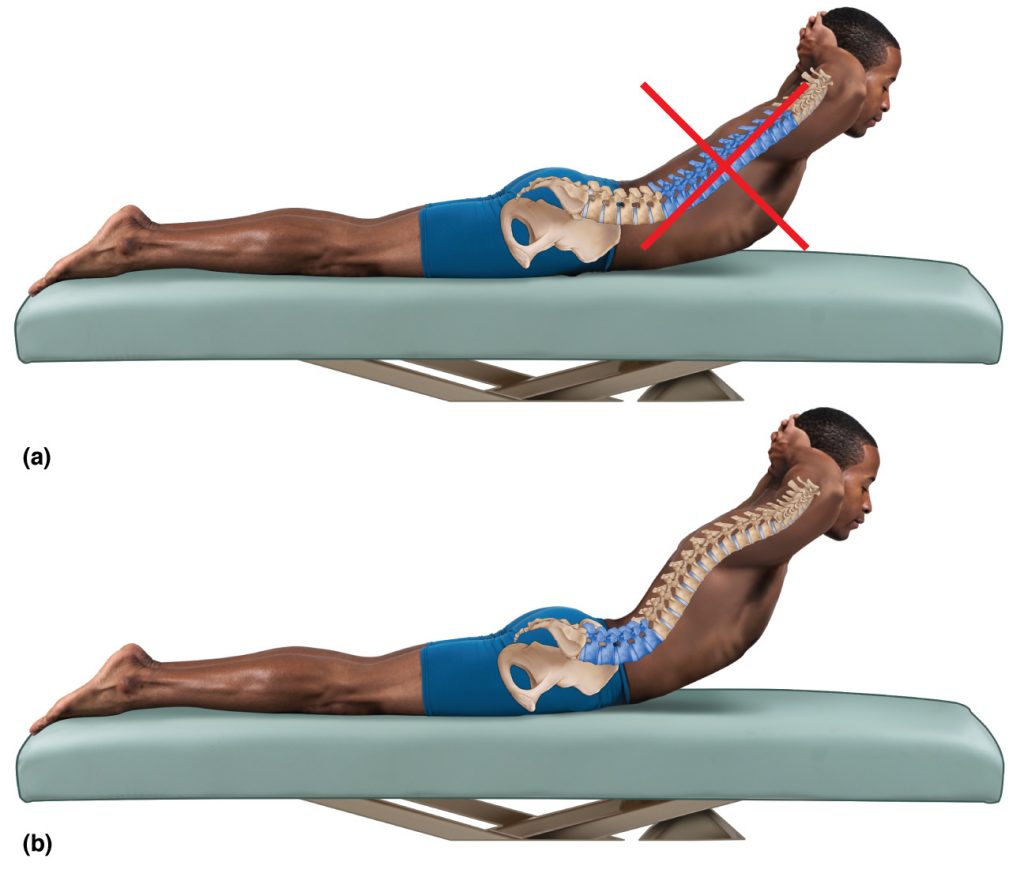
Figure 11. Extension exercise for a hypolordotic lumbar spine. The motion should not be occurring at the thoracic spine (A). Rather it should be initiated from the lumbar spine (B). Permission Joseph E. Muscolino.
Rehabilitating a lumbar hypolordosis requires the introduction of extension into the lumbar spine. Therefore extension exercises should be done with the initiation of motion lower in the lumbar spine instead of the thoracic spine (Figure 11).
Frontal Plane Stretching and Strengthening
Similar to altered sagittal plane postures, when the client has a frontal plane spinal dysfunction, in other words, a scoliosis, it is important to not just simply recommend lateral flexion stretching to one side and/or the other; it is important to instruct the client how to focus the stretching/strengthening exercise to the specific region of the spine based on its lateral flexion dysfunction.
Scoliosis
A right-convexity scoliotic curve of the spine is effectively a curve of left lateral flexion. Therefore it should be stretched into right lateral flexion. Similarly, a left-convexity scoliotic curve is a curve of right lateral flexion and therefore must be stretched into left lateral flexion. When a client presents with a scoliotic curve in one region of their spine, the stretch must be focused on that region. This is especially true if the client has an S-shaped scoliotic curve in which there are scoliotic curves in both directions.
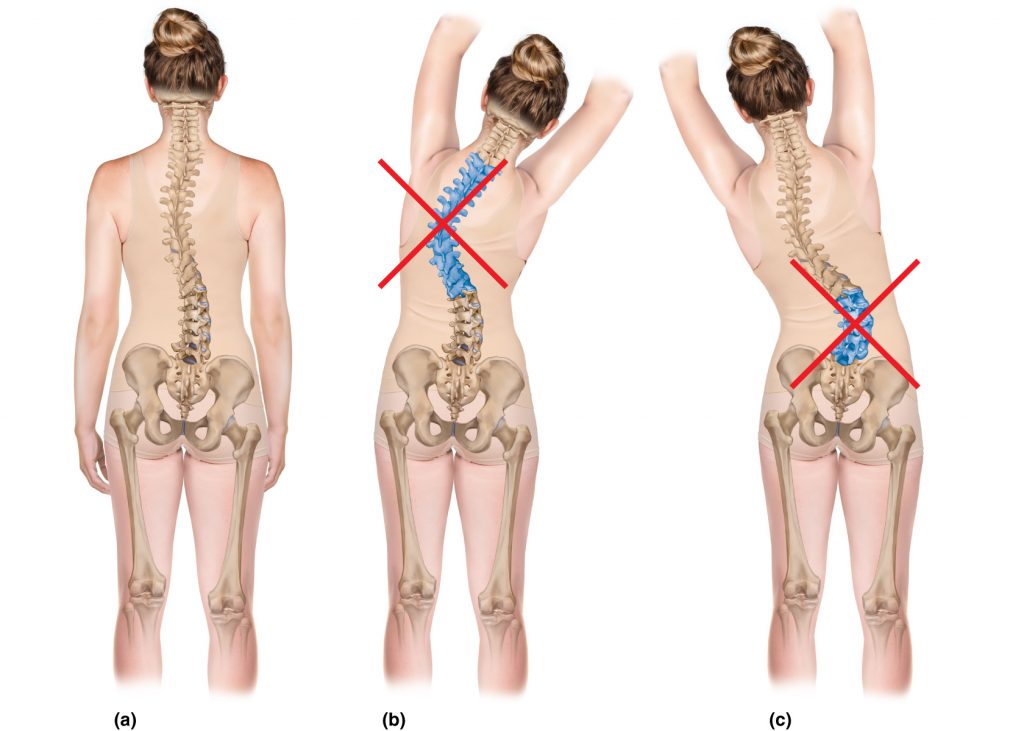
Figure 12. Non-specific stretching of the scoliotic spine. A, Right convexity lumbar scoliosis and left convexity thoracic scoliosis. B, Right lateral flexion stretch that increases the thoracic scoliotic curve. C, Left lateral flexion stretch that increases the lumbar scoliotic curve. Permission Joseph E. Muscolino.
For example, if the client has a right-convexity in the lumbar spine and a left convexity in the thoracic spine as seen in Figure 12A, simply asking the client to right laterally flex their spine will likely result in motion at the thoracic region instead of the intended target of the lumbar region. Not only will the stretch not decrease the lumbar scoliotic curve; it will actually increase the thoracic scoliotic curve (Figure 12B). And asking the client to left laterally flex the spine without specific directions will result in motion at the lumbar region instead of the thoracic region, again ineffectively addressing the intended target and worsening the other scoliotic curve (Figure 12C). Whether right lateral flexion or left lateral flexion is performed, each scoliotic curve will tend to compensate for the other scoliotic curve unless the client is directed to effect the stretch to the specific region of the spine needed.
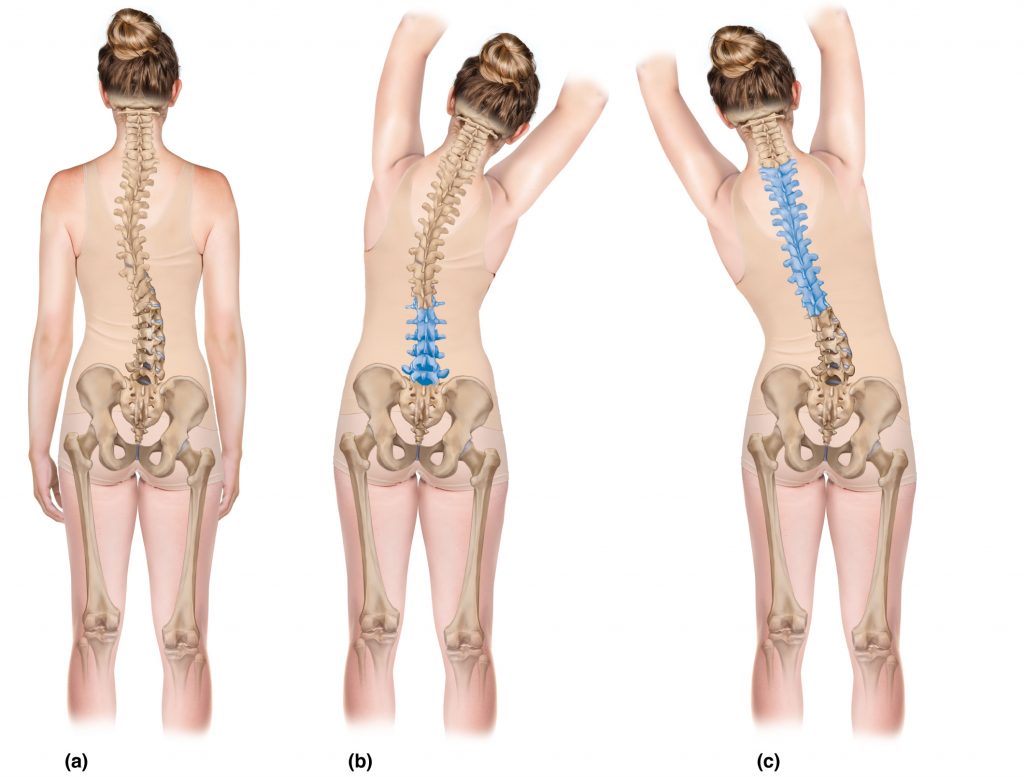
Figure 13. Specific stretching for scoliotic curves. A, Right convexity lumbar scoliosis and left convexity thoracic scoliosis. B, Right lateral flexion stretch that decreases the lumbar scoliotic curve. C, Left lateral flexion stretch that decreases the thoracic scoliotic curve. Permission Joseph E. Muscolino.
Therefore, the client needs to be instructed to initiate the stretching motion from the appropriate region of the spine. This can be challenging because the other opposite scoliotic curve will tend to move instead as seen in Figure 12. For this reason, cueing the client for proprioceptive feedback is important. Figure 13 demonstrates focused stretching that is appropriate for the client’s scoliotic curves. In Figure 13B, the client is right laterally flexing from the lumbar region to decrease the right-convexity lumbar scoliotic curve. Figure 13C demonstrates left lateral flexion stretching that is focused on the thoracic region to decrease the left-convexity thoracic scoliotic curve.
Transverse Plane Stretching and Strengthening
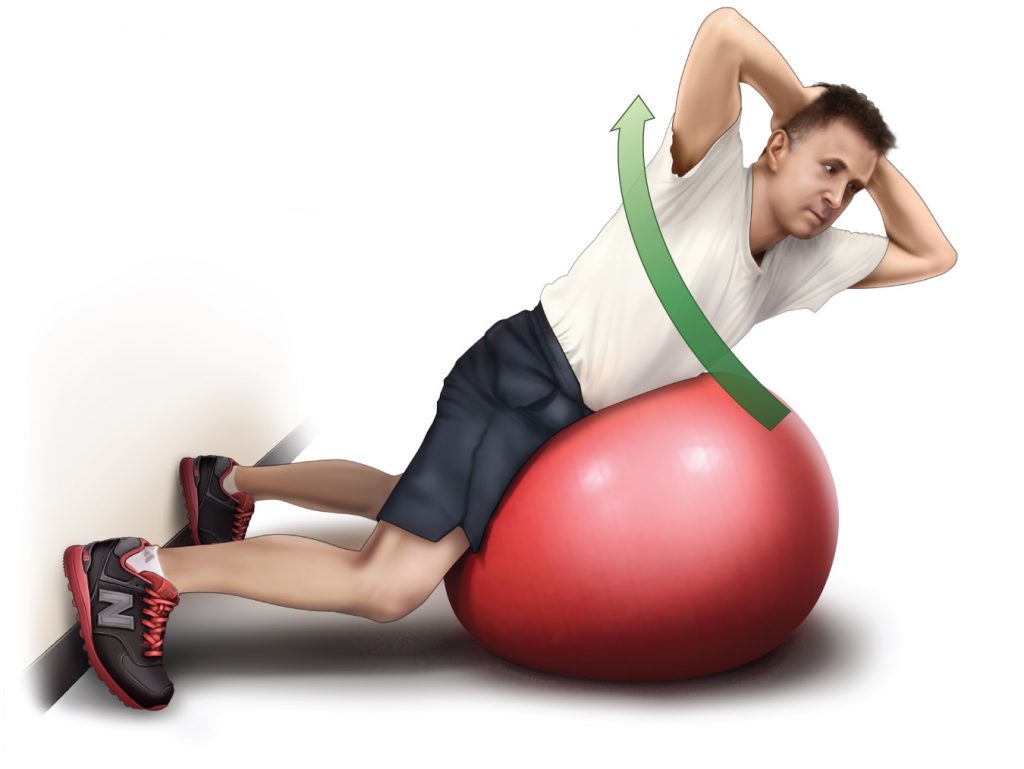
Permission Joseph E. Muscolino.
A scoliotic curve may be defined by its lateral flexion deformity; however, frontal plane lateral flexion always couples with transverse plane rotation. Therefore, it can be helpful to instruct the client to add in a transverse plane rotation component to their self-care stretching or strengthening exercise. For example, if it is noted that the client’s trunk is rotated to the left as a result of a scoliosis, then adding in right rotation to the exercise can help to correct the postural dysfunction. In the accompanying figure, the client is performing a strengthening exercise into extension on a gym ball, but instead of moving up perfectly into extension, the client is extending and right rotating the trunk.
Art by Giovanni Rimasti
Photography by Yanik Chauvin
This blog post article was originally published in the AMTA’s 2014 winter issue of the massage therapy journal.
