What Is the Coracobrachialis? (Quick Answer)
The coracobrachialis is a muscle in the anterior compartment of the (upper) arm. It attaches proximally on the coracoid process of the scapula and attaches distally on the medial shaft of the humerus. It performs flexion and adduction at the glenohumeral joint and serves as a key teaching muscle for core kinesiology concepts including open-chain vs. closed-chain movement, cardinal-plane vs. oblique-plane motion, and anatomic vs. non-anatomic actions.
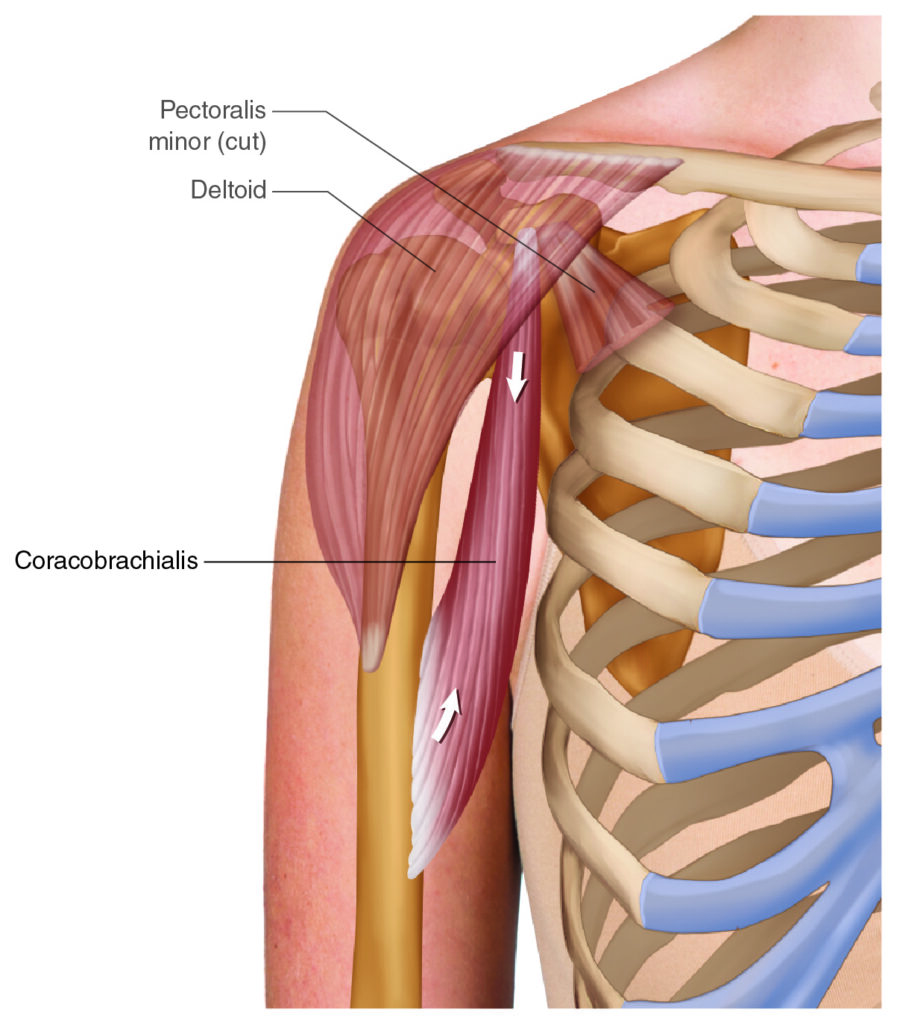
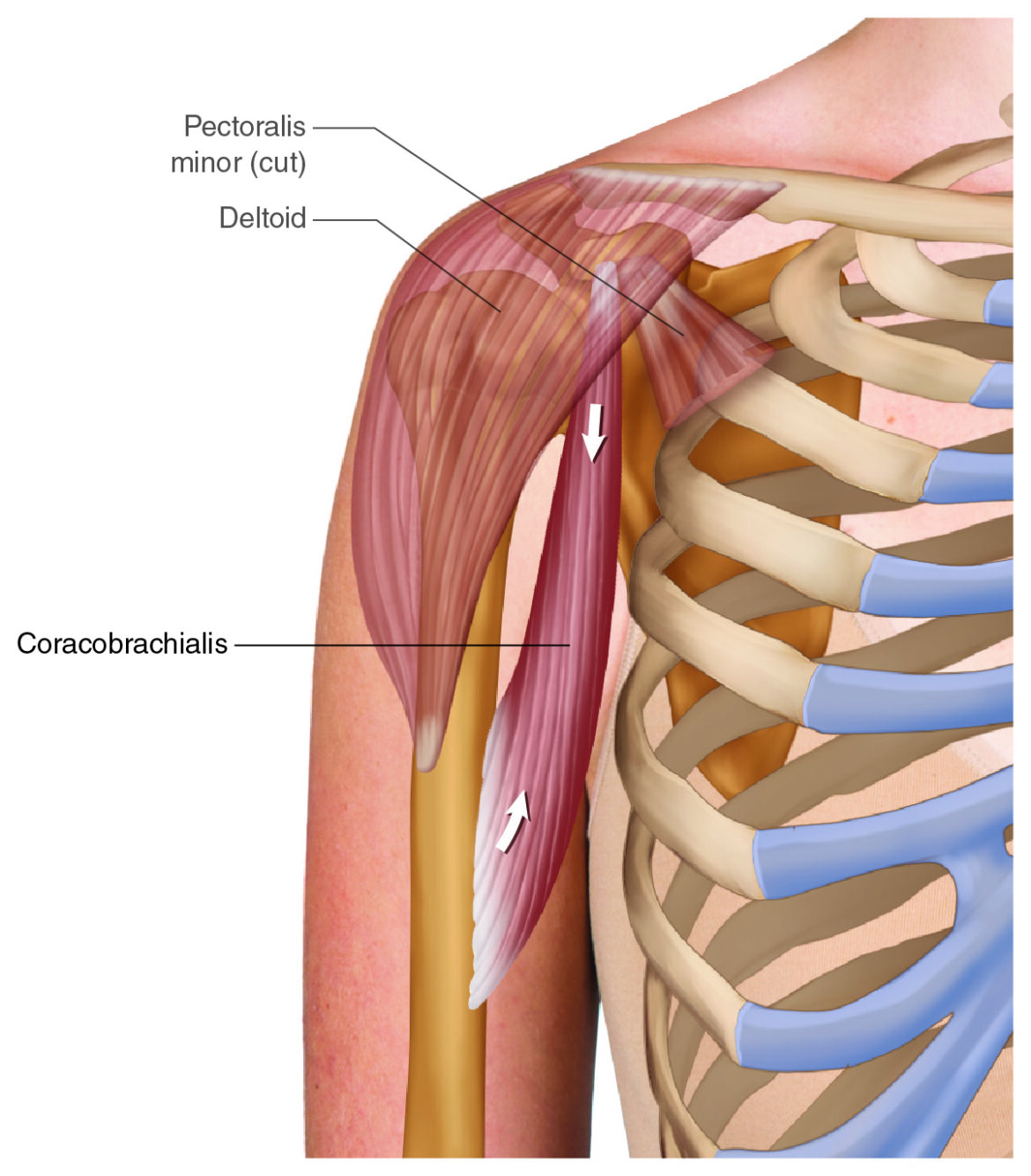
Coracobrachialis – Anterior View (Permission Dr. Joe Muscolino)
Introduction
The coracobrachialis is a muscle in the anterior compartment of the arm. More specifically, it is located anteromedially in the arm. It is a fascinating muscle to delve into because so many concepts of kinesiology (muscle biomechanics) can be explored.
Coracobrachialis Attachments
It attaches proximally onto the coracoid process of the scapula (origin), and distally onto the middle 1/3 of the medial shaft of the humerus (insertion).
At a Glance — Coracobrachialis Attachments:
- Proximal (origin): Coracoid process of the scapula
- Distal (insertion): Middle 1/3 of the medial shaft of the humerus
Coracobrachialis Joint Actions / Functions
The coracobrachialis is an excellent muscle to explore when it comes to its function, i.e., its movement patterns, because we have excellent examples of three fascinating concepts.
- What does it mean to create a cardinal-plane component joint action versus an oblique-plane (multiplane) motion pattern?
- What is an open-chain movement versus a closed-chain movement?
- And what is an anatomic action versus a non-anatomic action?
Let’s start with the open-chain joint actions of the coracobrachialis.
- The coracobrachialis crosses the glenohumeral (GH) joint anteriorly, so it flexes the arm at the GH joint in the sagittal plane.
- The coracobrachialis crosses the GH joint medially, so it adducts the arm at the GH joint in the frontal plane.
- If the arm is first abducted to 90 degrees, the coracobrachialis crosses the GH anteriorly so it can do horizontal flexion.
Cardinal-Plane Joint Action vs. Oblique-Plane Motion Pattern
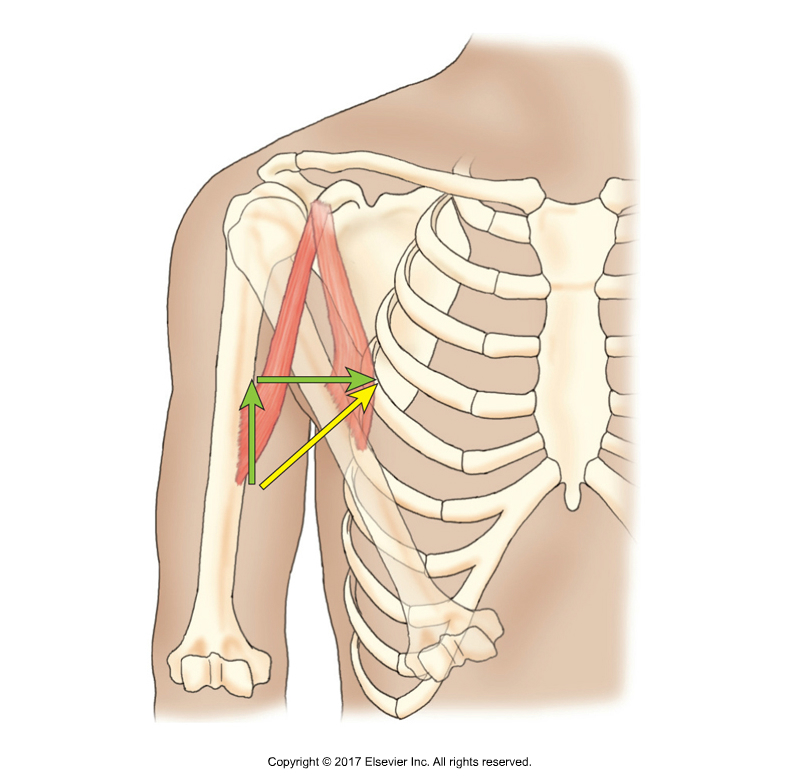
The coracobrachialis does “flexoadduction” of the arm at the GH jt. (Permission Dr. Joe Muscolino – Kinesiology textbook)
Let’s look at the actual (open-chain) movement/motion pattern that the coracobrachialis creates. The coracobrachialis has only one line of pull (it does not have one line of pull purely in the sagittal plane and another line of pull purely in the frontal plane). So, it cannot do pure sagittal-plane flexion nor can it do pure frontal-plane adduction. Its line of pull is within an oblique plane that is a combination of the sagittal and frontal planes, so its motion pattern would create a movement that is within that oblique plane, in other words, is a combination of flexion and adduction. I would love to call this motion “flexoadduction”, but we are not allowed to combine these joint action movement terms.
For this reason, a muscle atlas (including mine) would say that the coracobrachialis flexes and adducts the arm at the GH joint. The point is that “joint actions” are usually “cardinal-plane components” of a larger “oblique-plane motions.” Muscle atlases list these joint actions, but we need to remember that the actual motion pattern(s) that a muscle creates is based on its line of pull, which is usually in an oblique plane. For this reason, in my muscle atlas (The Muscular System Manual, 5th edition), I always additionally state the oblique-plane motion pattern for each muscle.
Open-Chain vs. Closed-Chain Movement
The next fascinating concept that we can explore with the coracobrachialis is the concept of an open-chain movement vs. a closed-chain movement. Open chain would be with the proximal (scapular, coracoid process) attachment fixed, and the distal (humeral) attachment mobile. We have already looked at the two open-chain joint actions of this muscle.
But what if the person’s hand is holding onto an immovable object? Then the distal arm would be fixed/stable, and the proximal shoulder girdle (scapula) would have to move instead. In a case like this, we would see the scapula downwardly rotate toward the humerus (in other words, origin moving toward the insertion). The bigger picture to be aware of is that when a muscle contracts, it pulls equally on both of its attachments; whichever is more mobile is the one that moves.
Anatomic Action
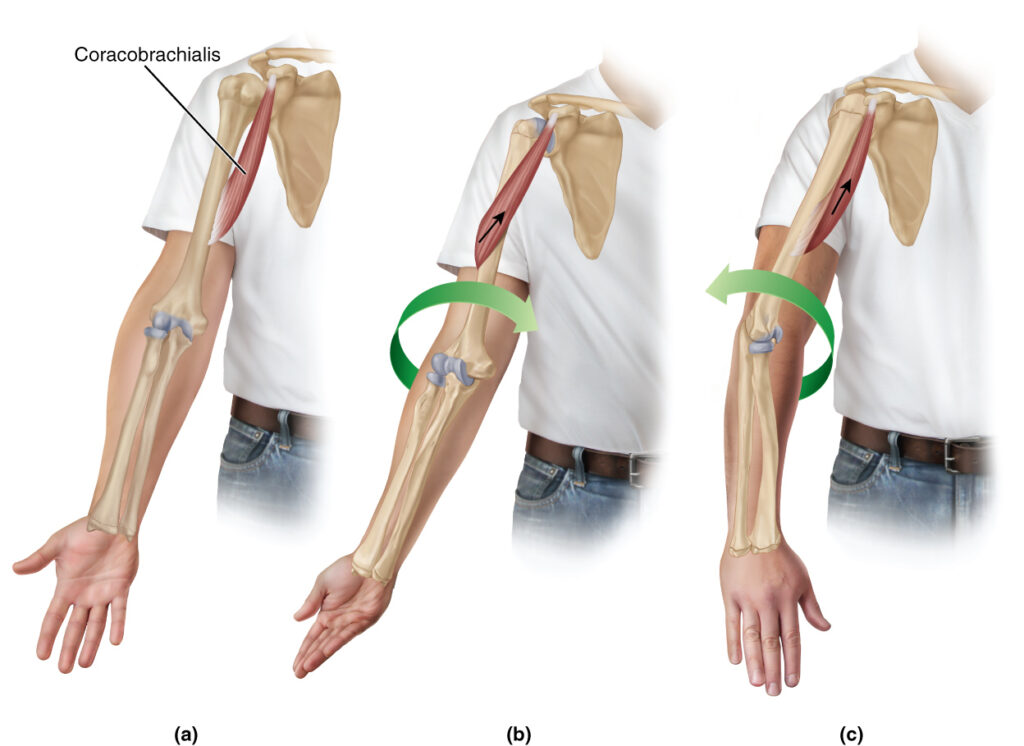
The coracobrachialis cannot rotate, can medially rotate, or can laterally rotate. Permission Dr. Joe Muscolino (learnmuscles.com)
The coracobrachialis is an excellent muscle to explore the idea of what an anatomic action is. In fact, most all joint actions that we learn are anatomic actions. As its name implies, an anatomic action is an action that the muscle can create when the muscle is in anatomic position. Looking at the coracobrachialis, we see that muscle atlases do not list rotation as one of its actions. That is because in anatomic position, the coracobrachialis does not have the ability to shorten and create rotation.
But, if the humerus were first in a position of lateral rotation, then when the muscle concentrically contracts and shortens (btw, all joint actions are concentric shortening
contractions), then the coracobrachialis would medially rotate the humerus at the GH joint. This can be seen by placing a large rubber band on the distal attachment of the coracobrachialis when the arm is laterally rotated, and pull that rubber band attachment toward the coracoid process of the scapula; the humerus will medially rotate. Likewise, if the arm were first in medial rotation, then the coracobrachialis would be able to laterally rotate the humerus to bring the two attachments closer together (again, you can demonstrate this with a large rubber band). So, the coracobrachialis can either medially or laterally rotate the humerus, or not rotate the humerus at all, depending on the position of the arm at the GH joint!
Because the coracobrachialis can laterally rotate a medially rotated humerus or medially rotate a laterally rotated humerus, sometimes it is referred to as a de-rotator muscle.
Frequently Asked Question: Does the coracobrachialis rotate the humerus? The coracobrachialis is not listed as a rotator in anatomic position. However, it can medially rotate a laterally rotated humerus, or laterally rotate a medially rotated humerus — making it a context-dependent de-rotator muscle.
Nearby Anatomy
Also attaching onto the coracoid process are the pectoralis minor and short head of the biceps brachii. In fact, the coracobrachialis and short head of biceps brachii always blend into each other. I have spent decades in cadaver labs and seen all sorts of anomalies in the musculature of the body, but I have never seen a coracobrachialis that was fully formed and separate from the biceps brachii short head; it always fuses/blends with the biceps brachii short head. For this reason, I often like to posit/joke that the coracobrachialis along with the two biceps brachii heads should be called the “triceps brachii”; of course, this can’t be done because there is already a triceps brachii on the posterior side of the arm.
Also, of note regarding adjacent structures, there are two major brachial plexus nerves (median and ulnar), and the brachial artery in the medial arm, very close to the coracobrachialis. And, more proximally in the arm, the musculocutaneous nerve pierces through the coracobrachialis. These are precaution areas when palpating and massaging the coracobrachialis.
Median nerve. Permission Dr. Joe Muscolino (learnmuscles.com).
Clinical Note — Neurovascular Precautions Near the Coracobrachialis:
- Median nerve
- Ulnar nerve
- Brachial artery
- Musculocutaneous nerve (pierces the muscle proximally)
Palpating the Coracobrachialis
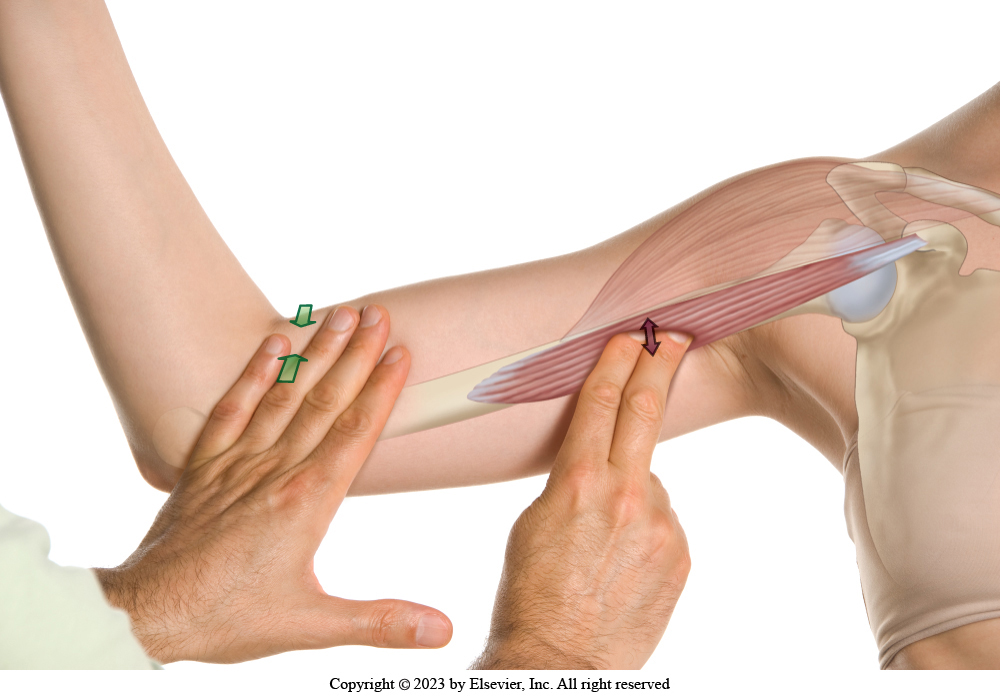
Palpation of the coracobrachialis with resisted horizontal flexion of the arm at the GH joint. (Permission Dr. Joe Muscolino – Muscle and Bone Palpation Manual)
The easiest and most efficient way to palpate the coracobrachialis is to have the client seated with their arm abducted 90 degrees at the GH joint and their forearm flexed 90 degrees at the elbow joint. This allows easy access into the medial arm where the coracobrachialis is located. It also allows us to differentiate GH joint movement from elbow joint movement.
Palpate in the medial arm (precaution: median and ulnar nerves and the brachial artery!), and feel for a pencil-thin, slender muscle that engages/pops and hardens when the client is resisted from performing horizontal flexion of the arm at the GH joint. What you feel will either be the coracobrachialis or the short head of the biceps brachii. How to discern which one it is? Now ask the client to try to flex their forearm at the elbow joint against your resistance and feel if the muscle you were just palpating engaged and hardened. If it did not, congratulations, you are on the coracobrachialis! You can now continue palpating it with resisted GH horizontal flexion from one attachment to the other. If what you were on does engage and harden with resisted elbow joint flexion, then you are on the biceps brachii short head, so you need to move slightly posterior to be on the coracobrachialis, and search for another thin muscle that engages with resisted GH horizontal flexion.
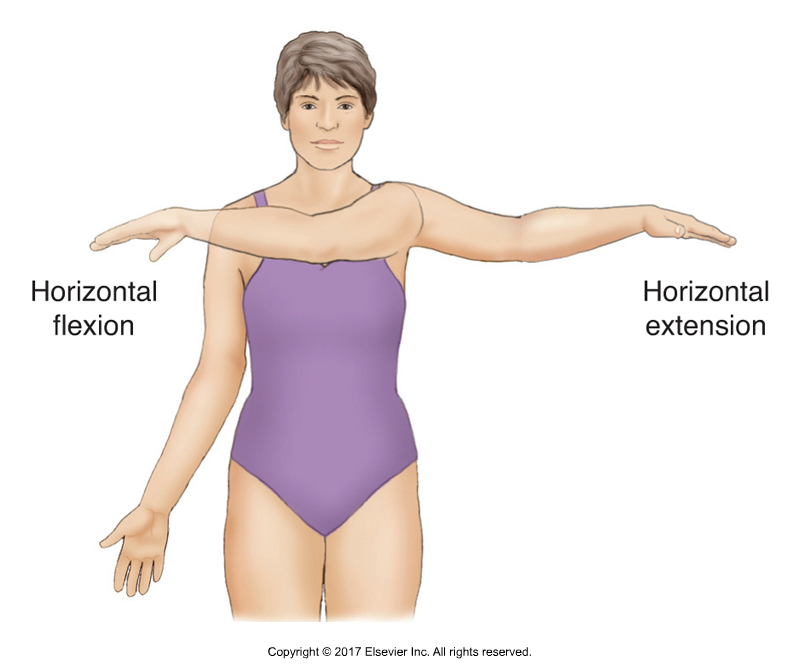
Horizontal flexion/extension of the left arm at the GH joint
Step-by-Step: How to Palpate the Coracobrachialis
- Seat the client with arm abducted 90° at the GH joint and forearm flexed 90° at the elbow.
- Palpate the medial arm (caution: nerves and brachial artery).
- Resist horizontal GH flexion — feel for a slender muscle that engages.
- Then resist elbow flexion — if the muscle does NOT harden, you are on the coracobrachialis.
- If it does harden, that is the biceps brachii short head; move slightly posterior to find the coracobrachialis.
Stretching the Coracobrachialis
One way to stretch the coracobrachialis is to bring the client’s arm into extension and abduction. These are simply the opposite movements of the joint actions of the coracobrachialis. Flexion and adduction are its concentric shortening joint actions, so extension and abduction would lengthen it.
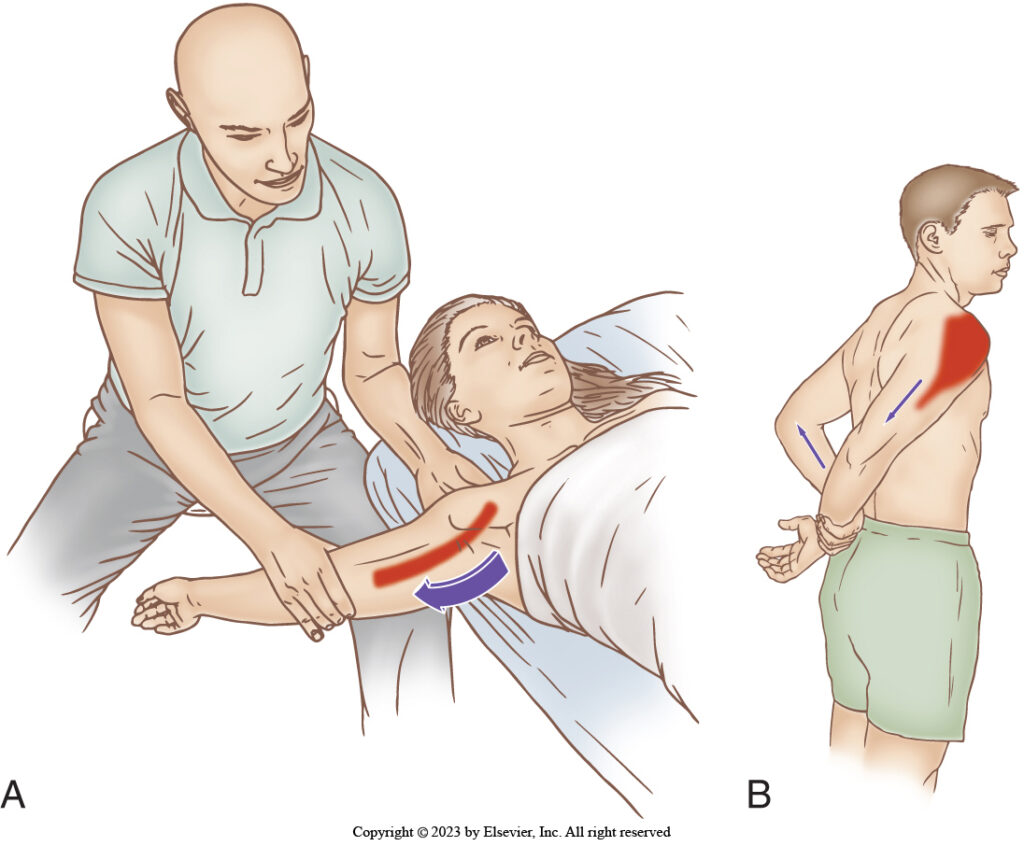
Stretching the coracobrachialis. Therapist-assisted and client self-care.
Another way to stretch the coracobrachialis would be to take advantage of the fact that it is a horizontal flexor. Simple stretch it with horizontal extension. And best to keep the forearm flexed so that the biceps brachii is slackened and knocked out of the stretch.
Coracobrachialis Stretch Options:
- Stretch 1: Arm into extension + abduction (opposite of its joint actions)
- Stretch 2: Horizontal extension with forearm flexed (also opposite of one of its joints actions, and to isolate from biceps brachii)
Massaging the Coracobrachialis
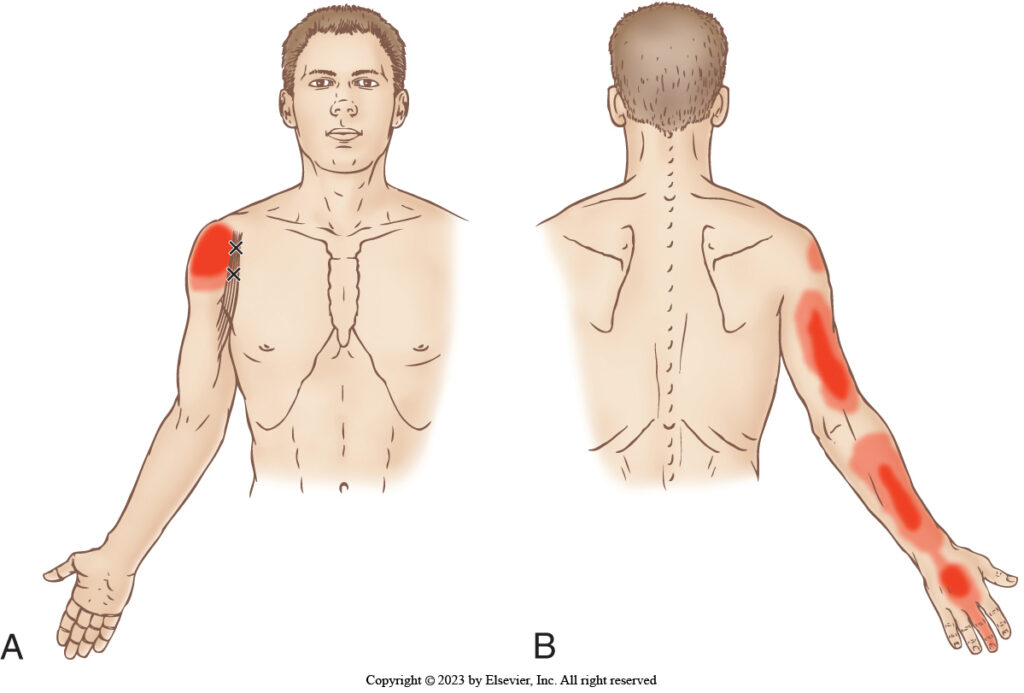
Coracobrachialis trigger points and referral zones (Permission Dr. Joe Muscolino – Muscle and Bone Palpation Manual)
Massaging the coracobrachialis follows from the assessment palpation. Once we have palpated and located it, assess for tightness and/or myofascial trigger points (TrPs). Be sure to work it from its humeral attachment, all the way to its attachment on the coracoid process of the scapula. Be aware of the precautions of not pressing into the brachial artery (of you feel a pulse, move a bit off it). And be aware to not press into the median and ulnar nerves (if the client feels an electric-shock type of feeling shoot down their upper extremity into their hand, move a bit off that spot), and not press into the musculocutaneous nerve (if the client feels an referral into the lateral forearm, move a bit off that spot). And keep in mind if you are continuing to palpate it with our protocol above, when you get more proximal, the coracobrachialis will blend into the biceps brachii, so it will be a harder to discern between them.
Conclusion
The coracobrachialis muscle is not usually on the radar of most manual therapy practitioners, but it is an important muscle to know for many reasons. Beyond its own importance in that it can become tight and painful like any muscle can, it is fascinating because it allows us to explore many concepts of kinesiology (muscle biomechanics) that increase our ability to understand and critically think in the world of muscles and manual therapy!

Dr. Joe Muscolino
Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com,
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
Frequently Asked Questions (FAQs)
Q: Where is the coracobrachialis located? A: The coracobrachialis is located in the anterior compartment of the (upper) arm, more specifically anteromedially.
Q: What are the attachments of the coracobrachialis? A: It attaches proximally to the coracoid process of the scapula (origin) and distally to the middle third of the medial shaft of the humerus (insertion).
Q: What does the coracobrachialis do? A: The coracobrachialis flexes and adducts (and horizontally flexes) the arm at the glenohumeral joint. It can also function as a de-rotator muscle depending on the arm’s starting position.
Q: How do you palpate the coracobrachialis? A: With the client’s arm abducted 90° and forearm flexed 90°, palpate the medial arm and resist GH horizontal flexion. If the muscle does not engage with resisted elbow flexion, you are on the coracobrachialis. If it does, you are on the biceps brachii short head; move slightly posteriorly to find the coracobrachialis.
Q: How do you stretch the coracobrachialis? A: Stretch it by bringing the arm into extension and abduction, or by using horizontal extension with the forearm flexed to isolate it from the biceps brachii.
