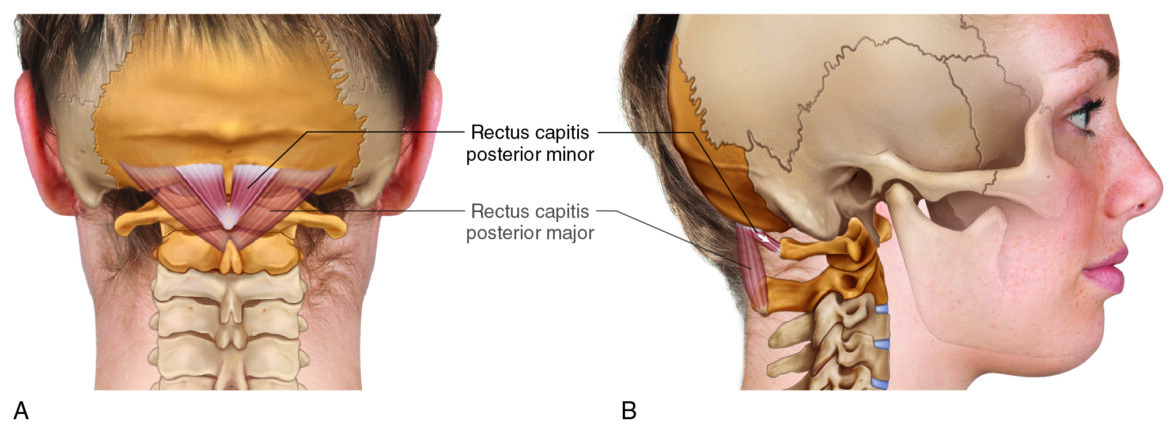
Rectus capitis posterior minor. In the lateral view, note the horizontal line of pull of the muscle. Permission Dr. Joe Muscolino (learnmuscles.com).
Introduction
The rectus capitis posterior minor is one of the four suboccipital muscles and one that is intimately related with tension headaches. It is also involved with the postural distortion pattern known as forward head posture, which is part of a larger postural distortion pattern known as upper crossed syndrome.
Rectus Capitis Posterior Minor Attachments
The rectus capitis posterior minor (RCPMin) attaches from the atlas/C1 (origin) to the occiput (insertion).
More specifically, the RCPMin attaches from the…
posterior tubercle of the atlas
to the
medial half of the inferior nuchal line of the occiput
Rectus Capitis Posterior Minor Functions
The RCPMin crosses the atlanto-occipital joint (AOJ) posteriorly, so one would think that it extends the head upon the atlas at the AOJ. However, its line of pull is nearly perfectly horizontal (which you can only appreciate with a lateral view), so it actually has another function. It pulls its more posterior attachment, the head, toward the more anterior attachment, the atlas. This results in protraction (anterior translation) of the head at the AOJ.
It does have a slight vertical component to its line of pull, so it can contribute to extension of the head at the AOJ.
And it is slightly to the side, so it can also contribute to lateral flexion of the head at the AOJ.
Nearby Anatomy
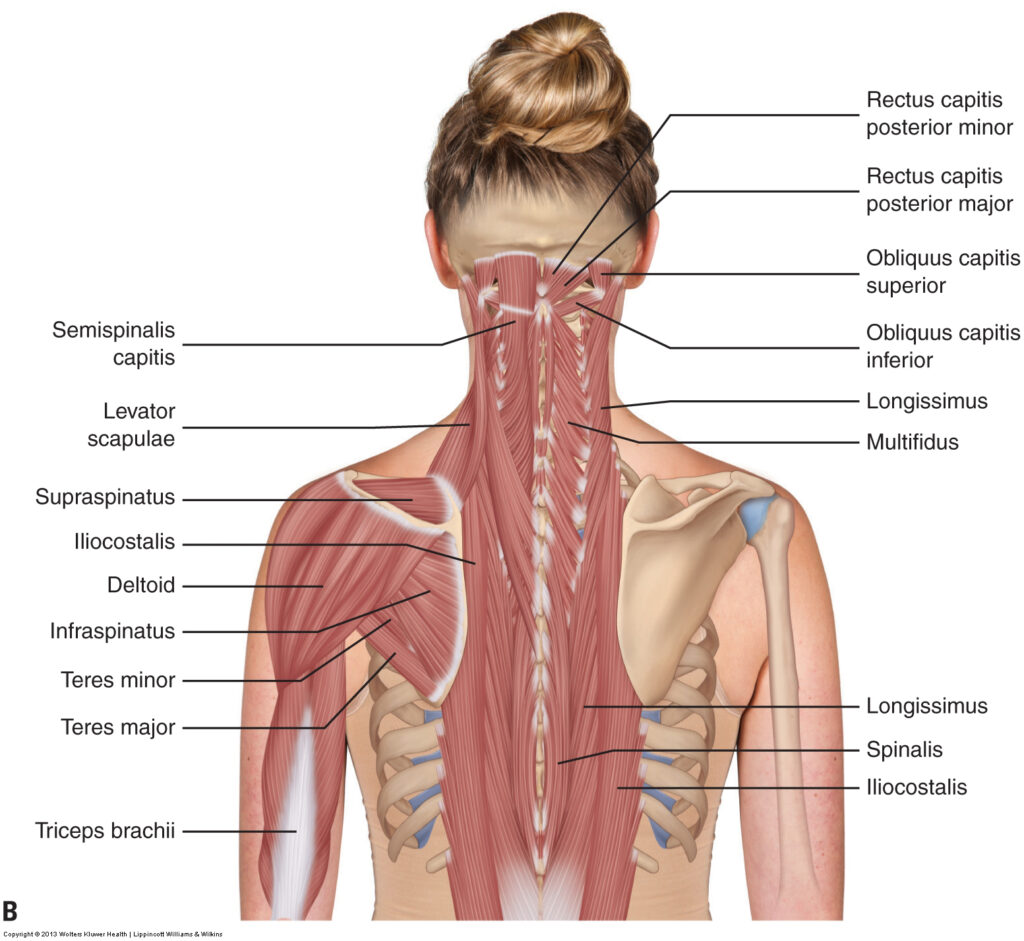
Permission Dr. Joe Muscolino (learnmuscles.com).
The RCPMin is directly medial to the rectus capitis posterior major (RCPMaj), another suboccipital muscle. It is also next to the obliquus capitis inferior (OCI), which is another of the four suboccipital muscles.
The RCPMin lies directly deep to the semispinalis capitis (of the transversospinalis group), which itself is deep to the upper trapezius.
Role in Headaches
The RCPMin, like any muscle in the back of the neck, can become tight and exert its pull on the fascia of the head, resulting in tension headaches. But the RCPMin has another particular relationship with headaches that was discovered relatively recently. In 1995, a paper was published in which the RCPMin was described as having an attachment directly into the tectorial membrane, an extension of the dura mater, one of the meninges of the brain. This attachment has been named the myodural bridge. The relevance is that if the RCPMin becomes tight, its tension/pulling force is exerted directly into the fascia of the brain, the dura mater, a very pain sensitive structure, which could cause a headache.
This is of particular importance to manual therapists, especially given how often this muscle is tight (hypertonic/overly facilitated/locked-short). The prevalence of this muscle to be tight is related to its role in the postural distortion pattern known as forward head posture, which itself is part of a larger dysfunctional pattern known as upper crossed syndrome.
Role in Forward Head Posture/Upper Crossed Syndrome
Forward Head Posture
If the RCPMin is tight and locked short, it will pull the head forward on the atlas (protraction at the AOJ).
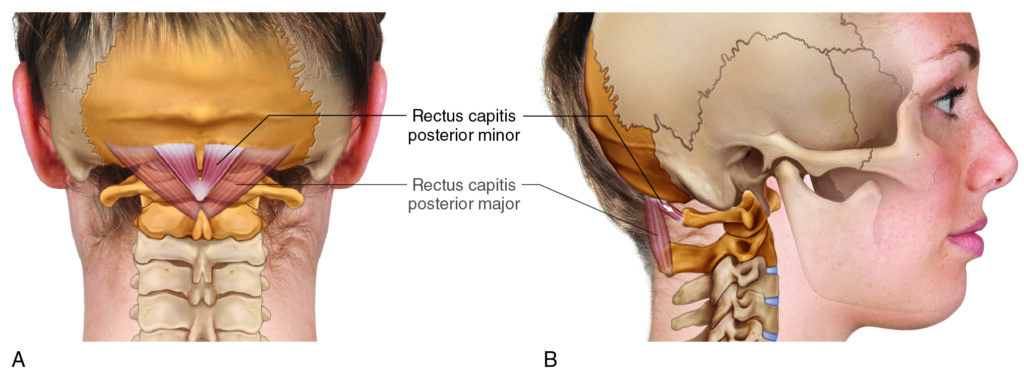
Rectus capitis posterior minor. Permission Dr. Joe Muscolino (learnmuscles.com).
This results in a forward carriage of the head, known as forward head posture. Conversely, if a person adopts a forward head posture habitually, the RCPMin will be short and slackened, but in time, will become adaptively short and tight (locked short). Hence, we have a classic chicken-and-egg vicious-cycle scenario. The more someone carries their head forward, the tighter this muscle becomes; the tighter this muscle becomes, the more entrenched will be the forward head posture.
The problem with forward head posture is that the center of weight of the head is forward of the trunk, over thin air, therefore the head is imbalanced forward such that it should fall into flexion. To counter this, the extensor musculature in the back of the neck (cervicocranial musculature) must isometrically contract. This constant isometric contraction of muscles in the back of the neck can then cause tension headaches because of their constant pull on the fascia of the head.
And this is in addition to the direct pulling force via the myodural bridge (described above) that can cause headaches.
Upper Crossed Syndrome
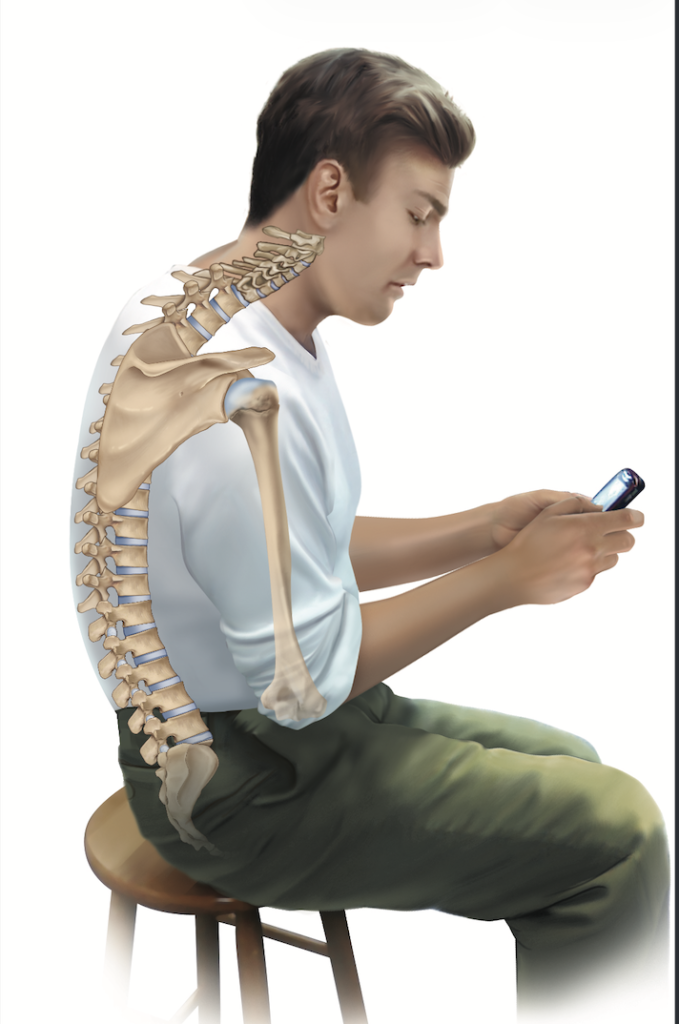
Upper Crossed Syndrome posture. Permission Dr. Joe Muscolino (learnmuscles.com).
Forward head posture is often found as part of a larger postural distortion pattern known as upper crossed syndrome. Upper crossed syndrome is marked by hyperkyphosis of the thoracic spine, which then results in hypolordosis (reduced extension) of the lower cervical spine, and hyperextension and protraction of the head at the AOJ. As a part of this, the shoulder girdles are overly protracted; and the arms (humeri) are overly medially rotated.
And, as a part of these skeletal distortion patterns, we have the tautening of the posterior fascial tissues, and also the associated locked-long and locked-short musculature, including the locked-short RCPMin.
Palpating the Rectus Capitis Posterior Minor
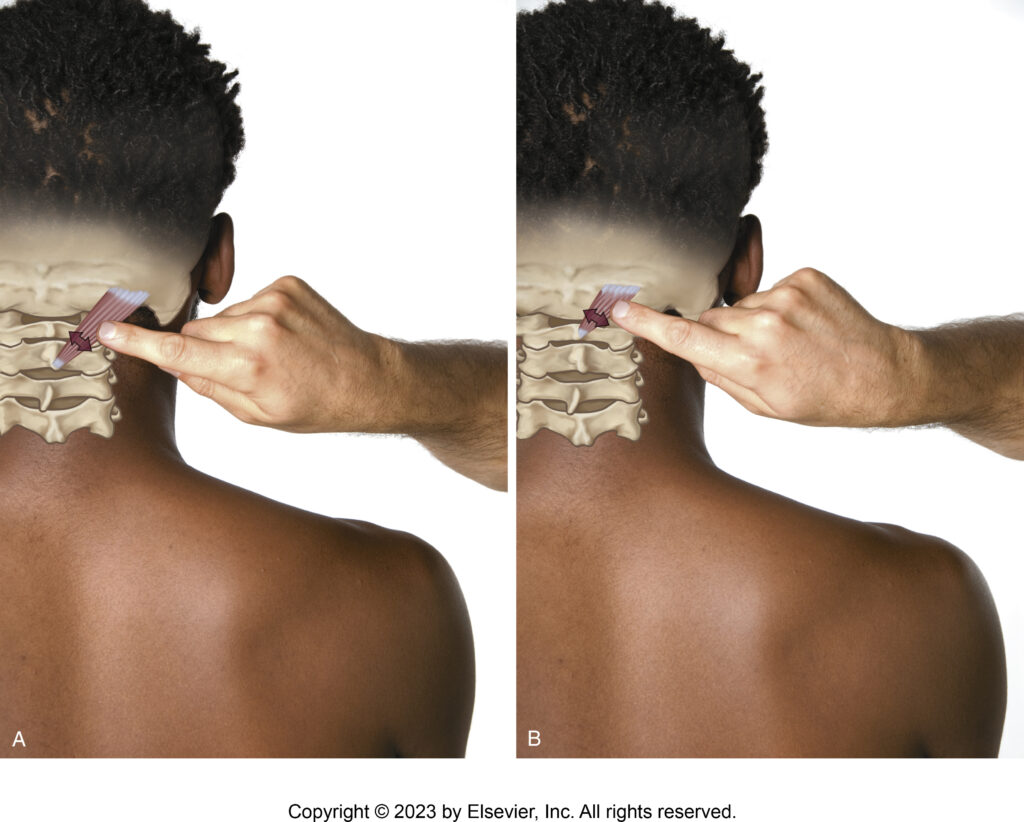
Palpating the rectus capitis posterior major (Figure A) and rectus capitis posterior minor (Figure B). Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The RCPMin is quite deep so it can be challenging to palpate and discern from adjacent myofascial tissue. Of specific concern is the more superficial semispinalis capitis muscle, which is the thickest muscle in the posterior neck. If this muscle is tight at baseline tone, which it often is when the client has forward-head posture, it can be very difficult to palpate through it to access the RCPMin. If, on the other hand, the semispinalis capitis is loose, then it is relatively easy to palpate and discern the RCPMin.
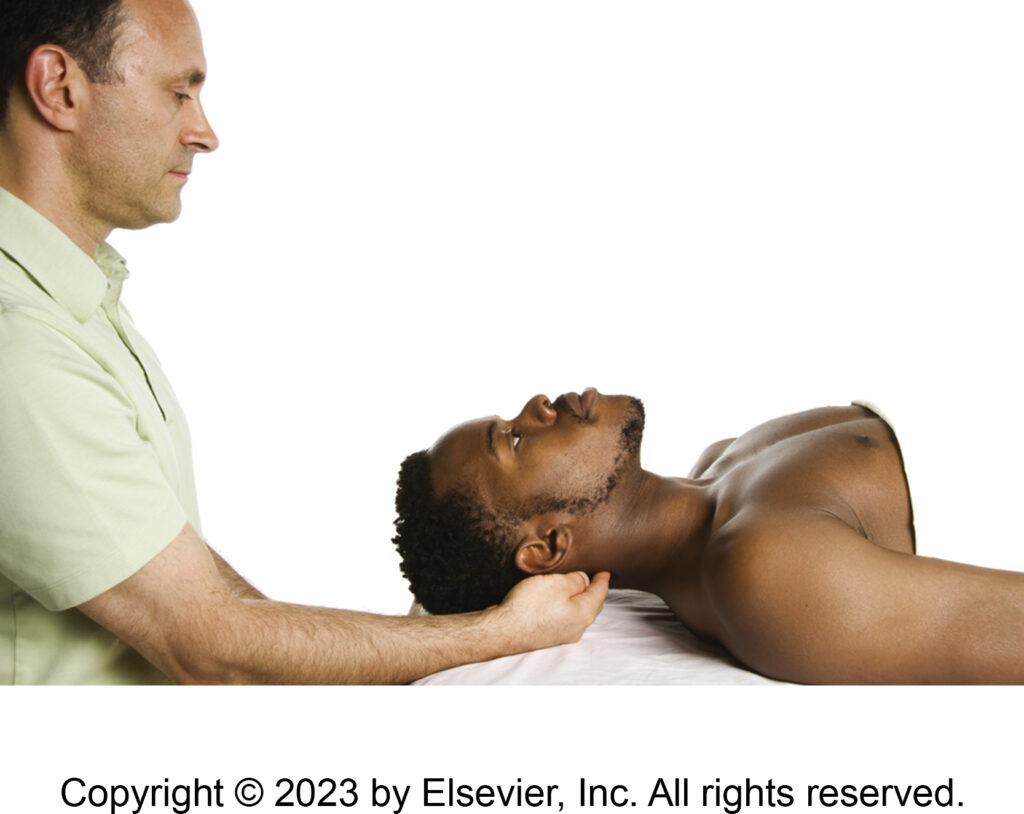
Indicating the location of the rectus capitis posterior minor of the suboccipital group for palpation. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
Have the client supine on the table. Find the external occipital protuberance (EOP); drop immediately inferior into the gap between the occiput and the large spinous process of C2 (the axis). There, if you carefully sink into the tissue, you will feel the relatively-small posterior tubercle of the atlas, which is the inferior attachment of the RCPMin. Drop immediately lateral and a bit superior and you will be over the RCPMin (deep to the upper trapezius and semispinalis capitis).
To try to palpate and assess the RCPMin, strum perpendicular to its direction of fibers. It runs from inferomedial on the atlas to superolateral on the occiput, so strum from superomedial to inferolateral across it. If it is tight, and the semispinalis capitis is sufficiently loose, then you should be able to palpate and discern the RCPMin as you strum perpendicularly, like strumming a guitar string.
Stretching the Rectus Capitis Posterior Minor
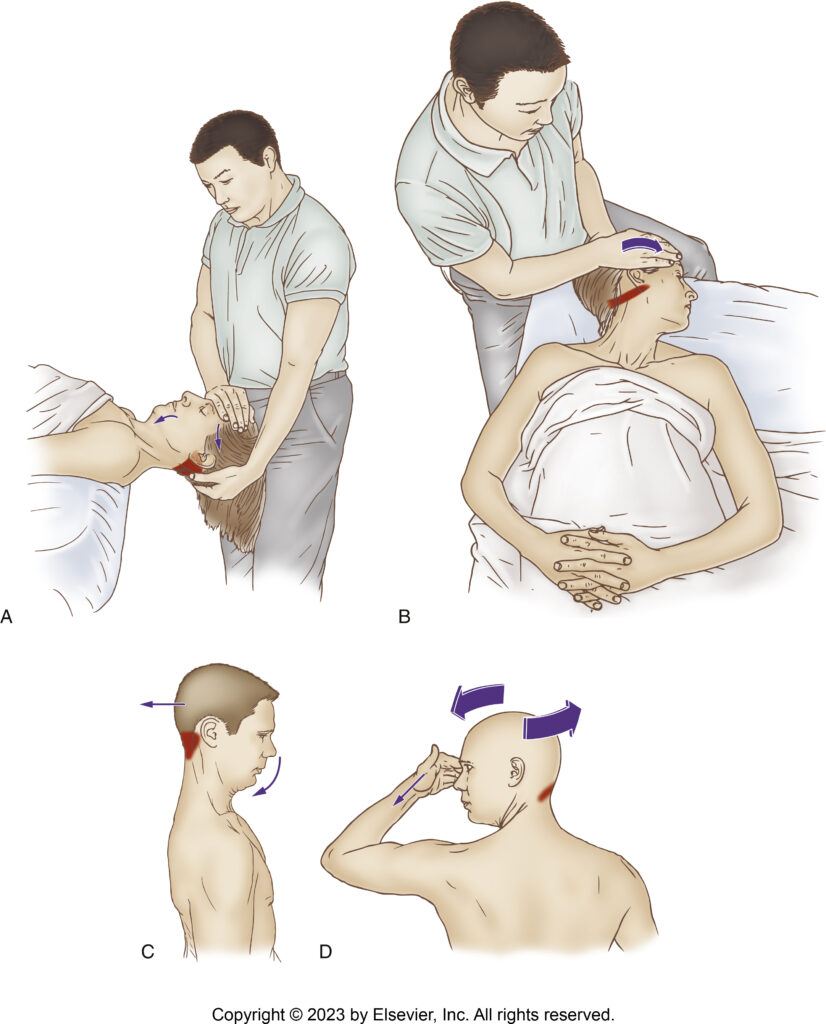
Stretching suboccipital musculature. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The RCPMin is a challenging muscle to stretch because the stretch movement is very small and must be precisely directed between the head and atlas. Given it is a protractor of the head, we need to retract the head as seen in Figures A and C in the accompanying illustration.
Massaging the Rectus Capitis Posterior Minor
Even if we cannot palpate and discern with certainty the RCPMin, we can still massage it with deeper pressure. The challenge, as with any deep muscle, is if the more superficial muscle (in this case the semispinalis capitis) is very tight, it is hard to translate our pressure through it into our target muscle, the RCPMin. If this is the case, we might need to work the client’s semispinalis capitis for a number of sessions to sufficiently loosen it so that our pressure better translates into the RCPMin.
Generally, for the RCPMin, I recommend cross-fiber strokes, so they need to be administered from superomedial to inferolateral, if seated at the head of the table and working with the client supine; or from inferolateral to superomedial, if working standing with the client prone. If it is hard to administer strokes across the muscle because it pulls the client’s hair, then static pressure can be used instead.
Note: Given how deep this muscle is located, our pressure must also be deep. Whenever working with deep pressure, it is important to first warm up the client’s tissues; and then when the deeper pressure is applied, sink in slowly and work with the client’s breath.
Conclusion
The rectus capitis posterior minor (RCPMin) is, clinically, one of the more important muscles in the human body, so it is especially important for manual therapists to be conversant with this muscle so that effective palpation assessment and massage and stretching treatment can be performed.
Biography

Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com.
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
Frequently Asked Questions About the Rectus Capitis Posterior Minor
What is the rectus capitis posterior minor?
The rectus capitis posterior minor (RCPMin) is one of the four suboccipital muscles. It attaches from the posterior tubercle of the atlas (C1) to the medial half of the inferior nuchal line of the occiput, and is intimately related with tension headaches and forward head posture.
How does the rectus capitis posterior minor cause headaches?
The RCPMin can cause tension headaches in two ways: by becoming tight and pulling on the fascia of the head, and via the myodural bridge — a direct attachment into the dura mater (one of the pain-sensitive meninges of the brain) first described in 1995.
What is the myodural bridge?
The myodural bridge is a direct attachment between the rectus capitis posterior minor and the tectorial membrane, an extension of the dura mater. When the RCPMin becomes tight, its tension is exerted directly into the dura mater, which is a very pain-sensitive structure and can cause headaches.
What is the role of the rectus capitis posterior minor in forward head posture?
If the RCPMin is tight and locked-short, it pulls the head forward on the atlas (protraction at the atlanto-occipital joint), causing forward head posture. Conversely, habitual forward head posture causes the RCPMin to become adaptively short and tight, creating a vicious cycle.
How do you stretch the rectus capitis posterior minor?
Because the RCPMin is a protractor of the head, stretching it requires retraction of the head at the atlanto-occipital joint. The movement is very small and must be precisely directed between the head and the atlas.
