
Signs and symptoms
The most common symptom of shin splints is pain in the leg when walking (the gait cycle) or running. With anterior shin splints, the pain most often occurs at heel strike and from heel-strike to midstance when the tibialis anterior is contracting. With posterior shin splints, pain most often occurs at toe-off when the posterior plantarflexion musculature (e.g., tibialis posterior) is contracting. Pain is also evident when the involved musculature is palpated. If the condition is more severe, swelling is also palpable and/or visible. With anterior shin splints, the swelling occurs along the tibial attachment of the tibialis anterior (the lateral border of the proximal 2/3 of the tibia). Swelling of the posterior musculature is usually more difficult to assess, especially if the involved muscle is located deeper, such as the tibialis posterior.
Assessment/Diagnosis

Palpation of the tibialis anterior. Permission: Joseph E. Muscolino. The Muscle and Bone Palpation Manual – With Trigger Points, Referral Patterns, wand Stretching 3ed. (Elsevier), 2016.
Assessment/diagnosis of shin splints is based on physical examination and verbal history. During verbal history, the client/patient will usually report a repetitive activity that places excessive physical demand on the musculature of the leg; often running for anterior shin splints and/or dancing or some other sport that requires repetitive toeing-off for posterior shin splints.
For anterior shin splints, physical exam should include palpation of the tibialis anterior, as well as the rest of the dorsiflexor musculature in the anterior compartment of the leg. Tightness (including myofascial trigger points), pain, and/or swelling in the tibialis anterior, especially along the tibial attachment, are the most common physical findings. If you are unsure of the location of the tibialis anterior, it can be discerned during palpation by resisting an oblique-plane motion of dorsiflexion and inversion of the foot. Indeed, the manual resistance offered for palpation might also cause pain in the tibialis anterior, also indicative of anterior shin splints. If your office has sufficient space, ask the client/patient to walk up and down a hallway; the presence of pain at heel-strike or between heel-strike and midstance is positive for anterior shin splints.
Palpatory examination for posterior shin splints can be more challenging. If the client/patient is experiencing pain in the posterior leg, especially when toeing off during the gait cycle, palpate each of the muscles of the posterior compartments, paying special attention to the soleus and tibialis posterior. Palpation of the soleus can be done in the posterior leg, deep to the gastrocnemius. With the client/patient prone and the leg flexed to 90 degrees at the knee joint (to slacken and inhibit the gastrocnemius), ask the client/patient to plantarflex the foot against mild to moderate resistance and feel for the soleus to engage. Once located, palpate the entirety of the soleus from the posterior perspective, feeling for global tightness, myofascial trigger points, pain, and/or swelling. If pain is found, it is important to ask the client/patient if the pain is similar to the characteristic pain that he or she has been experiencing. Note: As with the tibialis anterior, the manual resistance given during palpation might also cause pain in the soleus. The soleus should also be palpated in the lateral leg and the medial leg where it is superficial; similar to the palpation protocol for the soleus posteriorly, deep to the gastrocnemius, have the knee joint flexed to 90 degrees and resist plantarflexion of the foot.
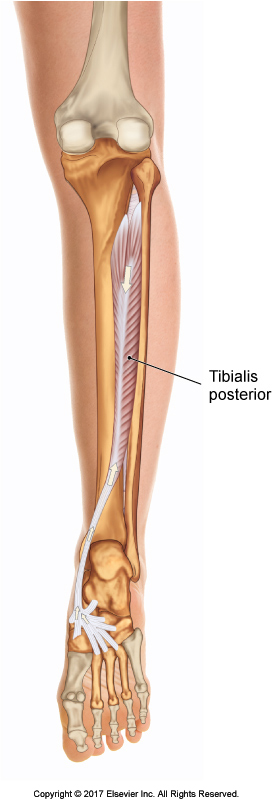
Posterior view of the tibialis posterior. Permission Joseph E. Muscolino. The Muscular System Manual – The Skeletal Muscles of the Human Body, 4ed (Elsevier) 2017.
Palpation of the tibialis posterior is more challenging. Even though a small part of it is superficial in the distal medial leg, its belly lies deep to the gastrocnemius and soleus, and to some degree the flexors digitorum and hallucis longus. With the client’s/patient’s knee joint flexed to 90 degrees and their foot passively slackened in plantarflexion, press gently but deeply into the midline of the posterior leg, feeling for tightness, the elicitation of pain, and or swelling deep in the posterior leg at the tibialis posterior. Discerning the tibialis posterior from adjacent musculature is challenging. Note: Whenever palpating deeply, it is important to sink in slowly and have the client/patient breathe.
X-Rays are not normally ordered for a soft tissue condition like shin splints. However, chronic shin splints might be detectable on X-Ray due to the changes at the periosteal attachment on the bone. X-Rays can also be valuable to rule out the presence of a tibial or fibular stress fracture.
Differential assessment
There are a number of conditions that offer a similar clinical picture to shin splints. Global tightness and/or myofascial trigger points in the involved musculature can also present with pain, especially with use and/or manual resistance to contraction of the muscle. Muscular strain will also present with pain as well as possible swelling. The key difference between these conditions and shin splints is the precise location of the pain; the primary source of pain with shin splints will be directly at the osseous attachment of the muscle on the tibia (or perhaps the fibula or the interosseus membrane). As stated, these other conditions often coexist with shin splints so the presence of one does not rule out the presence of the others; in fact, the presence of these other conditions increases the chance that shin splints will occur.
There are three other conditions that must be kept in mind when differentially assessing the client/patient for shin splints. The first is a stress fracture of the tibia or fibula. Stress fractures of the tibia are especially common and may present with all of the signs and symptoms of shin splints. As stated earlier, radiographic X-Ray examination is indicated if a stress fracture is suspected. It is also important to be sure that the client/patient does not have compartment syndrome of the deep posterior compartment of the leg or deep vein thrombosis. Each of these conditions would contraindicate some of the manual therapy approaches that would be used to treat shin splints.
