
Manual Therapy Treatment for Upper Crossed Syndrome

Stretching the shoulder girdle back into retraction. Permission Joseph E. Muscolino.
Given that upper crossed syndrome (named by Vladimir Janda) does not cause pain in the early stages, client/patients often do not present for treatment until with this condition is very chronic and progressed, and therefore stubborn and resistant to treatment. However, if consistent care is given, upper crossed syndrome responds very well to manual therapy. Moist heat, massage, and stretching should all be done to the facilitated/tight pectoralis musculature and SCM anteriorly and the extensor musculature of the neck (especially the upper trapezius and levator scapulae) posteriorly. Even though it is always wise to begin with light to medium pressure, transitioning to deeper pressure soft tissue manipulation is often necessary to break up long-standing fascial adhesions. At the tendons, cross fiber work should be performed. Soft tissue manipulation should also be performed to the inhibited musculature because chronic postural distortion can result in the build up of fascial adhesions in these muscles as well. If time permits, it is wise to work the lumbopelvic hip joint complex region as well, given that interplay between upper crossed syndrome and postural distortion patterns of the lumbopelvic region.
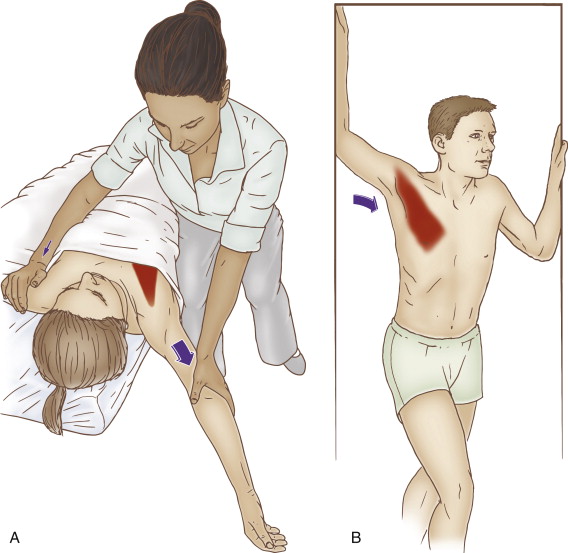
Therapist-Assisted and Self-Care Stretching of the Pectoralis Minor. Permission Joseph E. Muscolino. The Muscle and Bone Palpation Manual – with Trigger Points, Referral Patterns, and Stretching, 2ed (Elsevier, 2016).
For more stubborn cases, neural inhibition stretching techniques such as contract relax (CR; also known as post-isometric relaxation [PIR] and proprioceptive neuromuscular facilitation [PNF]) and agonist contract (AC; the basis for Aaron Mattes’ Active Isolated Stretching [AIS] technique) should be used. Especially effective for the pectoralis musculature is to use pin and stretch technique. With the client/patient supine and positioned toward the side of the table, pin the musculature with your finger pads as you bring the client/patient’s abducted arm off the side of the table and down into horizontal extension. Perform a number of repetitions of this procedure, each time changing the location of the pin pressure along the pectoralis musculature. To most effectively apply this technique to the pectoralis major, make sure that the client/patient’s scapula is stabilized on the table; to most effectively apply this technique to the pectoralis minor, have the client/patient move farther to the side so that their scapula is off the table and free to move.
Because any chronic postural dysfunctional pattern will eventually result in the presence of fascial adhesions in the ligament/joint capsule complex, mobilization of the glenohumeral joint and the thoracic and cervical spinal joints will most likely be beneficial and should also be done. For more chronic cases, mobilization of the thoracic spine into extension is usually critically important. Especially helpful is to use an extension break table with the client/patient supine, positioning different segmental levels of the thoracic spine over the break point of the table. If an extension break table is not available, a bolster can be placed under supine patient’s/client’s thoracic spine to mobilize it into extension.
As effective as heat, soft tissue manipulation, and stretching can be for upper crossed syndrome, the application of only these treatment modalities can never fully and permanently resolve the condition. The objective of these therapies is to loosen the tight musculature and other extra-articular and intra-articular taut soft tissues. However, that only addresses one half of the problem. The other half of each “arm of the cross” is the inhibited weakened musculature. To truly resolve upper crossed syndrome, these muscles must be strengthened. Therefore, referral to a fitness trainer, physical therapist, yoga or Pilates instructor, or the recommendation of specific exercises to strengthen the thoracic paraspinal extensors, scapular retractors, serratus anterior, and deep cervical flexors is imperative (for more on the strengthening of these muscles, see the self-care for the client/patient section to follow in a later blog post on this condition).
Summary of Manual Therapy Treatment Protocol for Upper Crossed Syndrome
| 1. Heat and then soft tissue manipulation to the pectoralis musculature |
| 2. Stretching (pin and stretch) to the pectoralis musculature |
| 3. Heat and then soft tissue manipulation to the posterior cervicothoracic region |
| 4. Stretching to the posterior cervicothoracic region |
| 5. Heat and then soft tissue manipulation to the GH medial rotators |
| 6. Stretching the GH medial rotators |
| 7. Mobilization of the glenohumeral and thoracic and cervical spinal joints |
| 8. Work the lumbopelvic/hip joint complex |
| 9. Strengthen (or refer out to strengthen) the weakened/inhibited musculature |
Precautions/Contraindications for Upper Crossed Syndrome
There are no specific precautions or contraindications when working on a client/patient with upper crossed syndrome other than being careful to not be overly forceful with both soft tissue manipulation pressure and stretching when working with the client/patient. It is important to be firm and assertive, but not aggressive.
