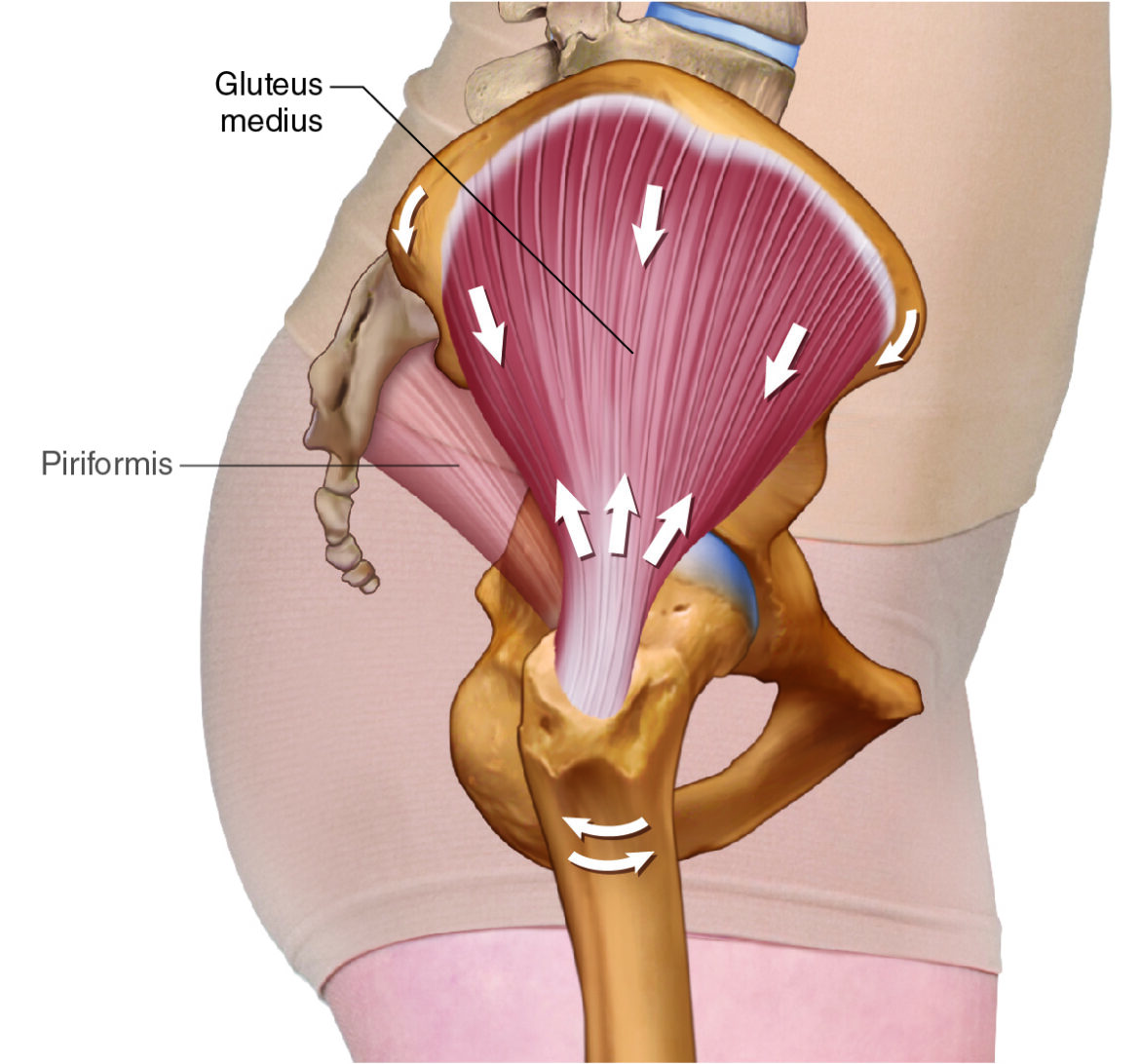
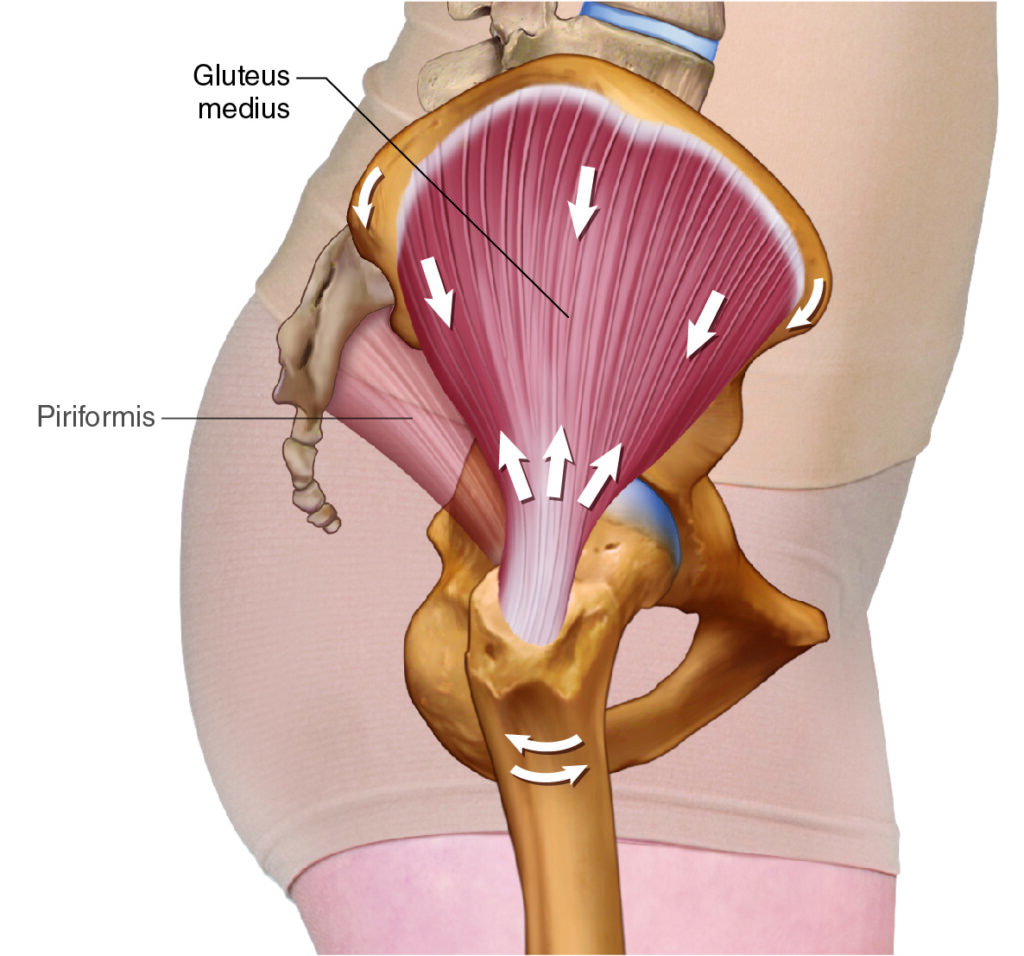
Gluteus medius – lateral view. Permission Dr. Joe Muscolino (learnmuscle.com).
Introduction
The gluteus medius is a fascinating muscle and one I like to call the Deltoid of the Hip because it has essentially the same structure and function at the hip joint that the deltoid has at the shoulder joint. They are both triangular in shape; the deltoid has anterior, posterior and middle sections; the gluteus medius has anterior, posterior, and middle sections. And each section of one muscle has the same actions as the corresponding section of the other muscle; the only difference being that the deltoid moves the arm at the shoulder joint, whereas the gluteus medius moves the thigh at the hip joint. Even their closed-chain actions are essentially the same, the deltoid acting on the scapula whereas the gluteus medius acts on the pelvic bone.
Gluteus Medius Attachments
The gluteus medius attaches from the ilium of the pelvic bone (origin) to the femur (insertion).
More specifically, it runs from…
the external aspect of the ilium (close to the iliac crest)
to the
lateral surface of the greater trochanter of the femur
Gluteus Medius Functions
Open-Chain
The anterior gluteus medius has essentially one line of pull that crosses the hip joint in the sagittal, frontal, and transverse planes, therefore it flexes, abducts, and medially rotates the thigh at the hip joint; the anterior deltoid flexes, abducts, and medially rotates the arm at the shoulder joint. The posterior gluteus medius extends, abducts, and laterally rotates the thigh at the hip joint; the posterior deltoid extends, abducts, and laterally rotates the arm at the shoulder joint. And the middle gluteus medius abducts the thigh at the hip joint; the middle deltoid abducts the arm at the shoulder joint.
In reality, each section, the anterior gluteus medius for example, cannot do pure flexion or pure abduction, or pure medial rotation of the thigh at the hip joint; instead because it has one line of pull across all three cardinal planes (sagittal, frontal, transverse), it must do an oblique-plane motion pattern that is the combination of all three of these cardinal-plane component joint actions. Similarly, the anterior deltoid must do an oblique-plane pattern of all three joints actions of flexion, abduction, and medial rotation at the shoulder joint.
It is fundamental in kinesiology terminology that a joint action is simply a cardinal-plane component of a larger oblique-plane (multiplane) motion pattern. The only time that a joint action is the motion pattern is when the muscle has only one line of pull and that line of pull is perfectly in one cardinal plane. For example, the brachialis in the arm has one line of pull perfectly in the sagittal plane and crosses the elbow joint, so its joint action of flexion of the elbow joint is its full motion pattern.
Closed-Chain
The gluteus medius is even more fascinating when we look at its closed-chain joint function at the hip joint. If the distal end of the kinematic chain of elements of the lower extremity (foot, leg, thigh, pelvis), therefore the foot, is stable, likely because it is against a stable surface like the ground in gait cycle, then the distal femoral attachment of the gluteus medius is fixed in place/stable, and the proximal iliac/pelvic bone attachment must move instead.
Therefore, when looking at the frontal-plane joint action of the gluteus medius in closed-chain mechanics, we see that instead of pulling the lateral surface of the thigh up toward the lateral surface of the pelvic bone (abduction of the thigh at the hip joint), the lateral surface of the pelvic bone is pulled down toward the lateral surface of the femur! This joint action is depression (also called lateral tilt) of the pelvic bone at the hip joint. In other words, depression of the pelvic bone at the hip joint is the closed-chain reverse action of abduction of the thigh at the hip joint. Similarly, we could see that anterior tilt of the pelvis at the hip joint is the closed-chain reverse action of the flexion of the thigh at the hip joint. And ipsilateral (same-side) rotation of the pelvis at the hip joint is the closed-chain reverse action of medial rotation of the thigh at the hip joint.
Closed-chain reverse actions are extremely common in the gait cycle (walking) in which a foot is on the ground (and not open to move freely in the air) 60% of the time. It is important to note that with closed-chain reverse actions, the origin moves toward the insertion. This is a good reason to abandon origin/insertion terminology, and instead simply describe muscle attachments anatomically, i.e., where they attach. Examples: proximal and distal, superior and inferior, or medial and lateral, or a mixture of superomedial to inferolateral.
The ability to compare the gluteus medius at the hip joint with the deltoid at the shoulder joint continues with their closed-chain actions. For example, the frontal-plane action of gluteus medius depressing the pelvis at the hip joint is analogous to the frontal-plane deltoid downwardly rotating the scapula at the shoulder joint.
Functional Importance of the Gluteus Medius
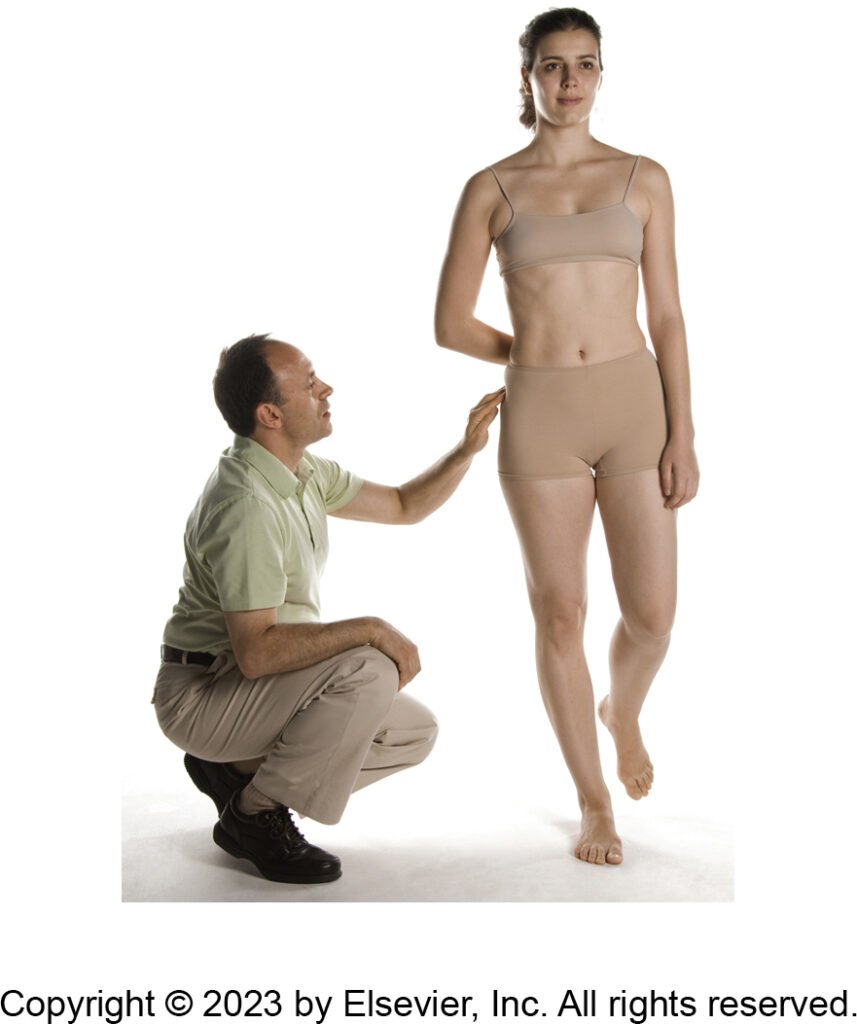
The gluteus medius engages isometrically on the support-leg side to stabilize the pelvis in the frontal plane. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The major functional importance of the gluteus medius is NOT to concentrically contract to move the thigh at the hip joint. It is NOT even to concentrically contract to move the pelvis at the hip joint. Its primary function is to isometrically contract to STOP the pelvis from moving in the frontal plane. If I lift my right foot off the floor so that I am standing only on my left leg/foot, then my pelvis should collapse to the right side because the center of my weight is unbalanced over thin air. This means that my pelvis would fall in the frontal plane (i.e., depress) to the right side. To stop the pelvis from falling to the right, the left-side gluteus medius isometrically contracts, creating a pulling force down on the left to prevent the pelvis from falling to the right.
So, when we are walking (or standing) and a foot leaves the ground to enter the swing phase, when walking for example, the gluteus medius on the stance-leg side must isometrically contract the entire time to stabilize the pelvis. For this reason, if a person spends a lot of time standing on one leg, or even placing more weight on one leg (perhaps simply a postural pattern, or perhaps due to asymmetry of dance choreography), the gluteus medius will become more developed on that side. OR, if due to an antalgic gait, perhaps due to a bad knee on one side, if we tend to weight bear more on the other side, we are using/overusing/misusing/abusing (to use Leon Chaitow’s famous verbiage) the gluteus medius on that side.
Nearby Anatomy
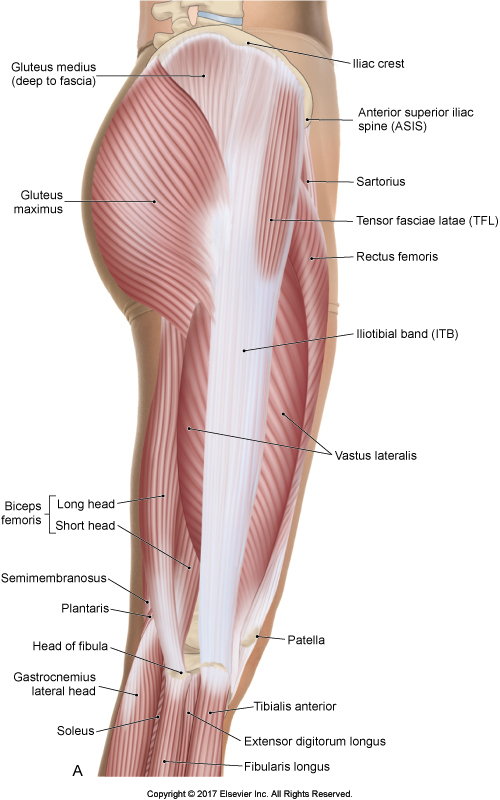
Superficial view of the right side. Permission Dr. Joe Muscolino – The Muscular System Manual 5ed.
The Gluteus medius spans from anterior to posterior across the lateral surface of the ilium of the pelvic bone. Anteriorly, it is deep to the tensor fasciae latae (TFL); posteriorly, it is deep to the gluteus maximus. But laterally, it is superficial, although it is deep to a layer of gluteal fascia. Posteriorly, where it is deep to the gluteus maximus, it sits proximal (superior) to the piriformis. Deep to the gluteus medius is the gluteus minimus.
Palpating the Gluteus Medius
Palpation of the gluteus medius. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The gluteus medius is fairly easy to palpate. Have the client side-lying so that we can palpate the opposite-side gluteus medius that is oriented toward the ceiling. You are standing behind the client. Find the midpoint of the iliac crest and drop immediately off it distally (inferiorly) and you will be on the gluteus medius.
Now ask the client to gently abduct the thigh at the hip joint and you should feel the gluteus medius engage and pop. Then ask the client to relax and re-place your fingers a baby step toward the greater trochanter, repeating the process. The key is to feel for the change in the texture from soft to hard to soft to hard. If there are taut fibers, they are generally running the length of the muscle and can be best palpated transversely (horizontally). Continue this process until you have palpated as much of the muscle as possible. Note, it can be challenging to palpate the fibers that are deep to the TFL and deep to the gluteus maximus.
Preferential palpation of the anterior and posterior fibers of the gluteus medius respectively. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The anterior fibers of the gluteus medius can be preferentially palpated with abduction plus flexion of the thigh; the posterior fibers can be preferentially palpated with abduction plus extension of the thigh. Once you have discerned the borders of the gluteus medius with this process, ask the client to remain relaxed and palpate to assess the health of the muscle at baseline tone.
Stretching the Gluteus Medius
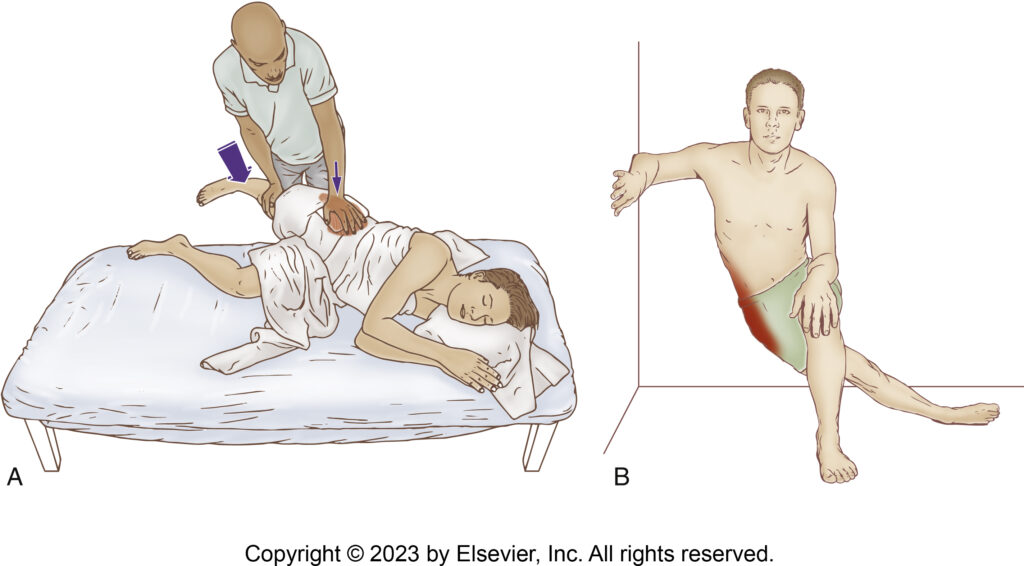
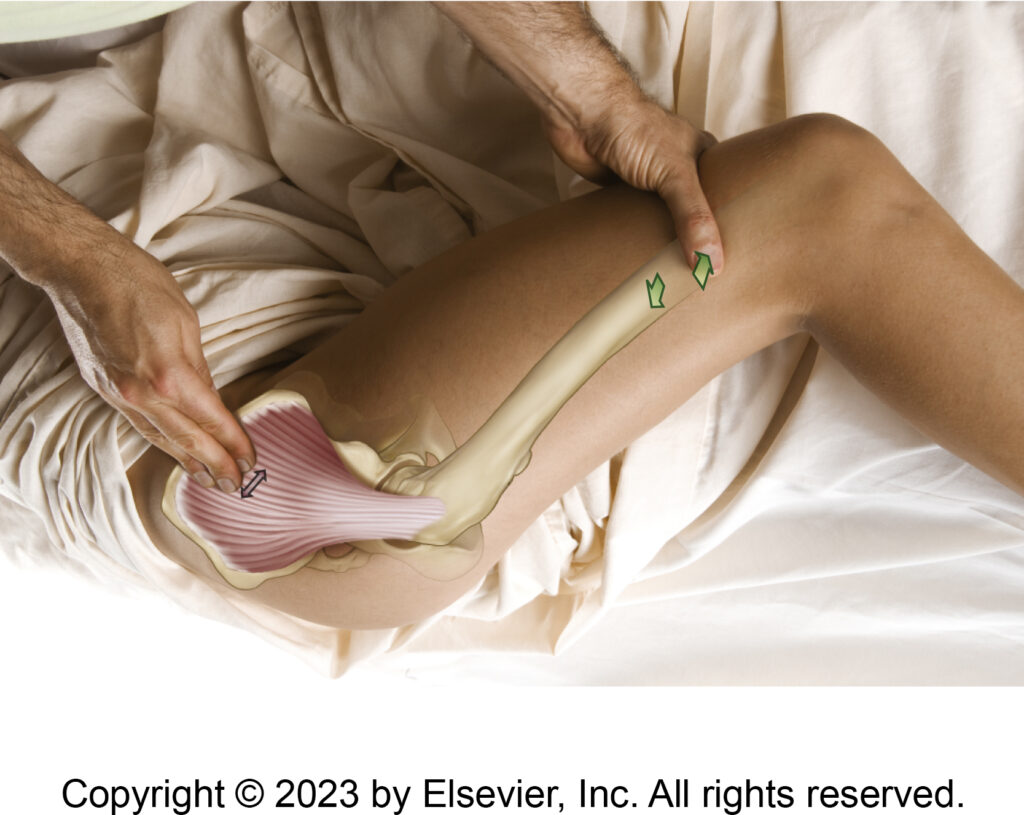
Stretching the gluteus medius. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
The gluteus medius is most easily stretched with the client in the same side-lying position that was used for palpation (as well as can be used for massage), and you are standing behind them. Given that stretching a muscle is making it longer, and that a joint action is a shortening concentric function, all we need to do when stretching a target muscle is do the opposite of its joint action.
So, given that the major joint action of the gluteus medius is abduction of the thigh at the hip joint, we stretch it with adduction of the thigh at the hip joint. The problem is that the other thigh (lower extremity) gets in the way, so, ask the client to position themselves diagonally on the table such at that their shoulder is far away from you, but their pelvis is close to you. This way, when you bring their thigh into adduction, it can fall down off the table without having its path obstructed by the other lower extremity or by the table.
Note, because the thigh is falling somewhat into extension behind the other thigh as it adducts down toward the floor, this protocol tends to preferentially stretch the more anterior fibers of the gluteus medius (because the anterior fibers are flexors as well).
Stabilization
Because this stretch force upon the gluteus medius will create tension in the muscle that will play out (pull) on the iliac crest attachment of the muscle, this stretch protocol would, if proper stabilization is not applied, result in the iliac crest simply depressing, and we would lose the stretch force into the muscle. So, it is important to stabilize the iliac crest. How? Simply get in the way of how it would end of moving. Or think of the stabilization as doing the opposite of what the muscle would do; it would depress on that side, so you need to apply a force on the iliac crest toward elevation on that side. Because pushing directly on the skin overlying the iliac crest could be uncomfortably for the client, a cushion should be used to spread out the force of the stabilization contact.
Massaging the Gluteus Medius
Gluteus medius trigger points and their referral zones. Permission Dr. Joe Muscolino – The Muscle and Bone Palpation Manual 3ed.
Massaging the gluteus medius is easy to accomplish with the client side-lying, and you standing behind them. For deeper work, make sure that the table is low enough that you can position your body weight above. Table height will vary tremendously depending on the contact you elect to use, from finger/thumb pads (table muscle to be low) to forearm contact (the table must be higher). Strokes can be longitudinal along the length of the fibers, usually most easily accomplished from proximal to distal, although they can be done distal-to-proximal. And work can be performed cross-fiber, from posterior to anterior.
Role in Trendelenburg Gait
The gluteus medius has a prominent role in a musculoskeletal condition known as Trendelenburg gait. Trendelenburg gait occurs when a person who is walking does not adequately stabilize their pelvis, so we see their pelvis fall to the side of the foot that is lifted with each step (swing-phase leg). This shows a weak or inhibited gluteus medius on the stance-leg side. This type of gait is often done purposely to draw attention to the pelvis and often used in modeling when walking on the catwalk.
It is important to note that even if a person voluntarily chooses to walk this way, if it is done habitually, in time, due to disuse, their gluteus medius could become weak and eventually unable to adequately stabilize the pelvis when walking so that the person will develop Trendelenburg gait as a dysfunctional movement pattern (and dropping the pelvis toward the swing-leg side will no longer be voluntary).
Role in Scoliosis
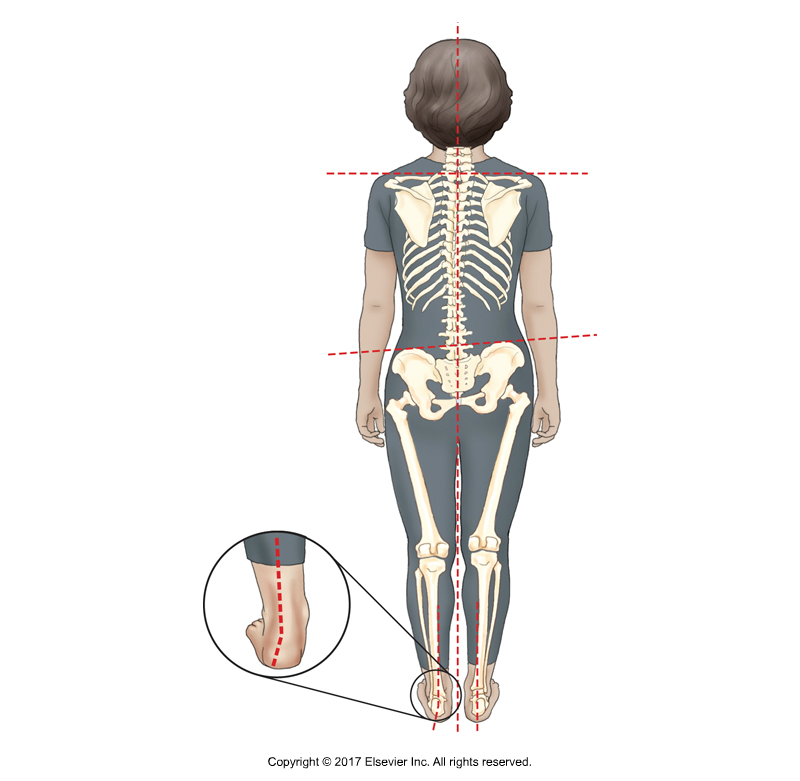
If the pelvis is low on one side for any reason (here a dropped arch), the spine must have a scoliotic curve to compensate and bring the head level. Permission Dr. Joe Muscolino – Kinesiology – The Skeletal System and Muscle Function 4ed.
If a gluteus medius on one side is chronically weak, it could allow a chronic posture of the pelvis dropping to the other side. Given that the top of the pelvis (the sacral base) is the pedestal upon which the lumbar spine sits, if this base is unlevel, then the lumbar spine will begin unlevel in the frontal plane; therefore L5 must begin unlevel to one side. If we eventually want our head to be level (which we do for vision and proprioception; it is called the righting reflex), then we must have a compensatory scoliosis to bring our head level.
Similarly, if a gluteus medius were to be too tight (hypertonic, overly facilitated, locked-short) at baseline tone, it would pull the pelvis down on that side, creating an unlevel pelvis (sacral base) in the other direction, thereby necessitating a compensatory scoliosis to bring the head level.
The point is that any asymmetry in frontal-plane musculature across the hip joint can create an unlevel pelvis resulting in a compensatory scoliotic curve. The gluteus medius is the most powerful frontal-plane muscle at the hip joint, so it is often implicated.
Take-Home Lesson…
If your client has a scoliotic curve, then the symmetry of baseline tone of the gluteus medius should be assessed, as well as any condition of the lower extremity that can create an obliquity in the frontal-plane posture of the pelvis.
Conclusion
The gluteus medius is an incredibly important muscle for many reasons. One is that it is so functionally important at the hip joint, especially with frontal-plane mechanics. And this can have implications with dysfunctional movement patterns (e.g., Trendelenburg gait) as well as postural distortion patterns of scoliosis.
And just as fascinating is to see the relationship between glute medius structure and function at the hip joint and compare it to the structure and function of the deltoid at the shoulder joint. Indeed, the gluteus medius can be described as the deltoid of the hip.
Biography

Dr. Joseph Muscolino, DC is a soft-tissue oriented chiropractic physician and leading educator in manual and movement therapy. He is the author of eight major textbooks published by Elsevier and LWW, translated into more than 10 languages and used worldwide in core curriculum and clinical practice. A global lecturer and NCBTMB-approved CE provider, he offers COMT (Clinical Orthopedic Manual Therapy) certification workshops across the US and internationally. Visit his website at: LearnMuscles.com.
LearnMuscles Continuing Education (LMCE) is one of his online subscription platforms with over 4,000 video lessons for manual and movement therapy professionals, and more than 320 free NCBTMB-CE hours.
