Shoulder Impingement Syndrome
This is the 3rd of 3 blog post articles on Shoulder Impingement Syndrome.
Shoulder impingement syndrome is a condition in which the distal tendon of the supraspinatus and the subacromial bursa (also known as the subdeltoid bursa) become impinged between the head of the humerus and the acromion process of the scapula. Sometimes the long head of the biceps brachii is also involved. There are a number of reasons that this condition can occur. Following are the six major causes of shoulder impingement syndrome.
- Medially Rotated Arm
- Weak Scapular Upward Rotators
- Tight Scapular Downward Rotators
- Weak Rotator Cuff Musculature
- Hypomobile Sternoclavicular Joint
- Shape of the Acromion Process
This article covers the last two in the list: hypomobile sternoclavicular joint & shape of the acromion process.
Hypomobile Sternoclavicular Joint
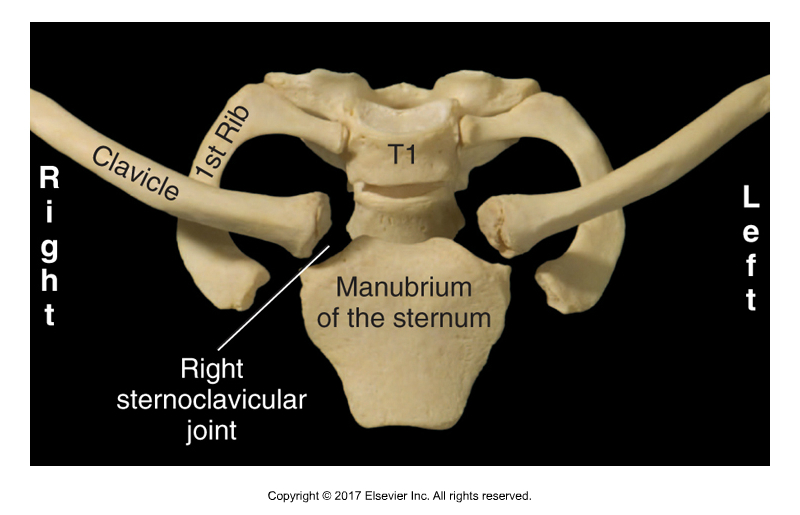
Sternoclavicular Joint. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. Elsevier, 2017).
Another reason for shoulder impingement syndrome to occur is insufficient elevation of the clavicle. Most of scapular upward rotation is actually caused by elevation of the clavicle at the sternoclavicular (SC) joint. The term scapulohumeral rhythm should really be called claviculo-scapulo-humeral rhythm. Therefore, if clavicular elevation is prevented for any reason, shoulder impingement syndrome can occur. Four possible reasons are tight clavicular depressors (e.g., pectoralis minor, pectoralis major, subclavius, latissimus dorsi, lower trapezius, lower fibers of serratus anterior), weak clavicular elevators (e.g., upper trapezius, levator scapulae, rhomboids, upper fibers of serratus anterior), arthritis of the SC joint, or joint hypomobile dysfunction of the SC joint. Note: during claviculo-scapulo-humeral motion, the clavicle must also upwardly rotate, therefore, the same arguments can be made for tight clavicular downward rotators (and/or weak clavicular upward rotators to be possible causes of impingement syndrome.
(Click here for the blog post article: What is Joint Mobilization?)
Shape of the Acromion Process
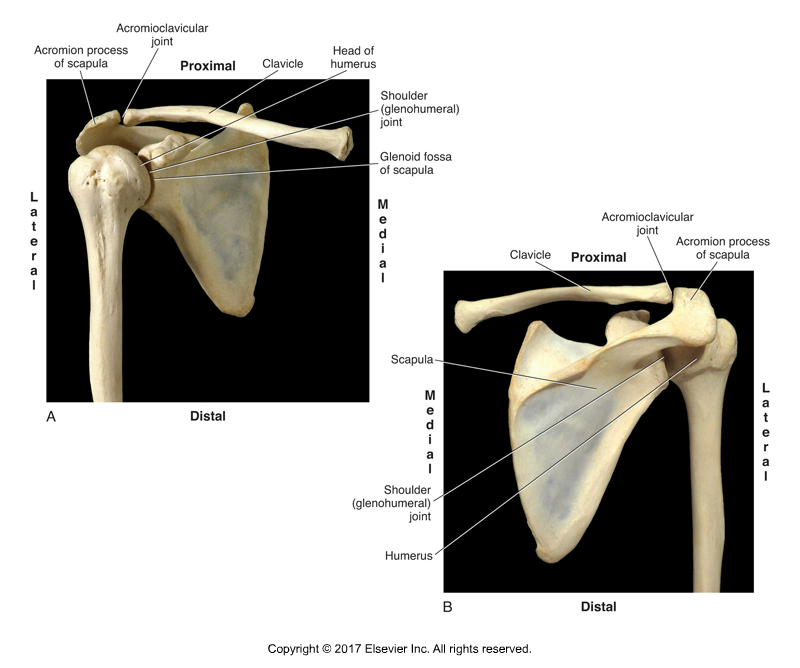
Acromion Process and Head of Humerus. Permission Joseph E. Muscolino. Kinesiology – The Skeletal System and Muscle Function, 3rd ed. Elsevier, 2017).
One more reason for shoulder impingement syndrome to occur is if the shape of the acromion process is such that it does not allow enough space for the head of the humerus to move upwardly unobstructed. For example, some people naturally have an acromion process that is downwardly sloped. Another reason is if there is an osteoarthritic bone spur at the distal end of the acromion process. When the deltoid contracts, it pulls on its acromion process attachment, and by Wolff’s Law, excessive pulling can cause the physical stress that can cause the bone spur to form. Therefore, people who overuse their deltoid often develop bone spurs at the distal end of the acromion process, leading to the increased possibility of shoulder impingement syndrome.
This is the 3rd of 3 articles on shoulder impingement syndrome.
The three articles are:
- Medially Rotated Arm & Weak Scapular Upward Rotators
- Tight Scapular Downward Rotators & Weak Rotator Cuff Musculature
- Hypomobile Sternoclavicular Joint & Shape of the Acromion Process
(Click here for the blog post article: What are the Causes of Frozen Shoulder?)
