Muscles of the Pelvis
This blog post article is an overview of the muscles of the pelvis. For more complete coverage of the structure and function of the low back and pelvis, The Muscular System Manual – The Skeletal Muscles of the Human Body, 4th ed. (2017, Elsevier) should be consulted.
Similar to learning the muscles of the lumbar spine/trunk, it can be helpful to first look at the functional groups of muscles of the pelvis when learning or reviewing them. Before doing that, it is important to first place muscles of the pelvis into their three major categories. They are:
- Muscles that attach from the pelvis to the trunk and cross the lumbosacral joint
- Muscles that attach from the pelvis to the thigh/leg and cross the hip joint
- Pelvic floor muscles that are located wholly within the pelvis
Note: Figures 30 through 32 are large group figures of the muscles of the trunk/pelvis/thigh for a bigger picture of the relationships between the muscles of this region (these same figures were shown in the last blog post in this series – they were Figures 16 through 18).
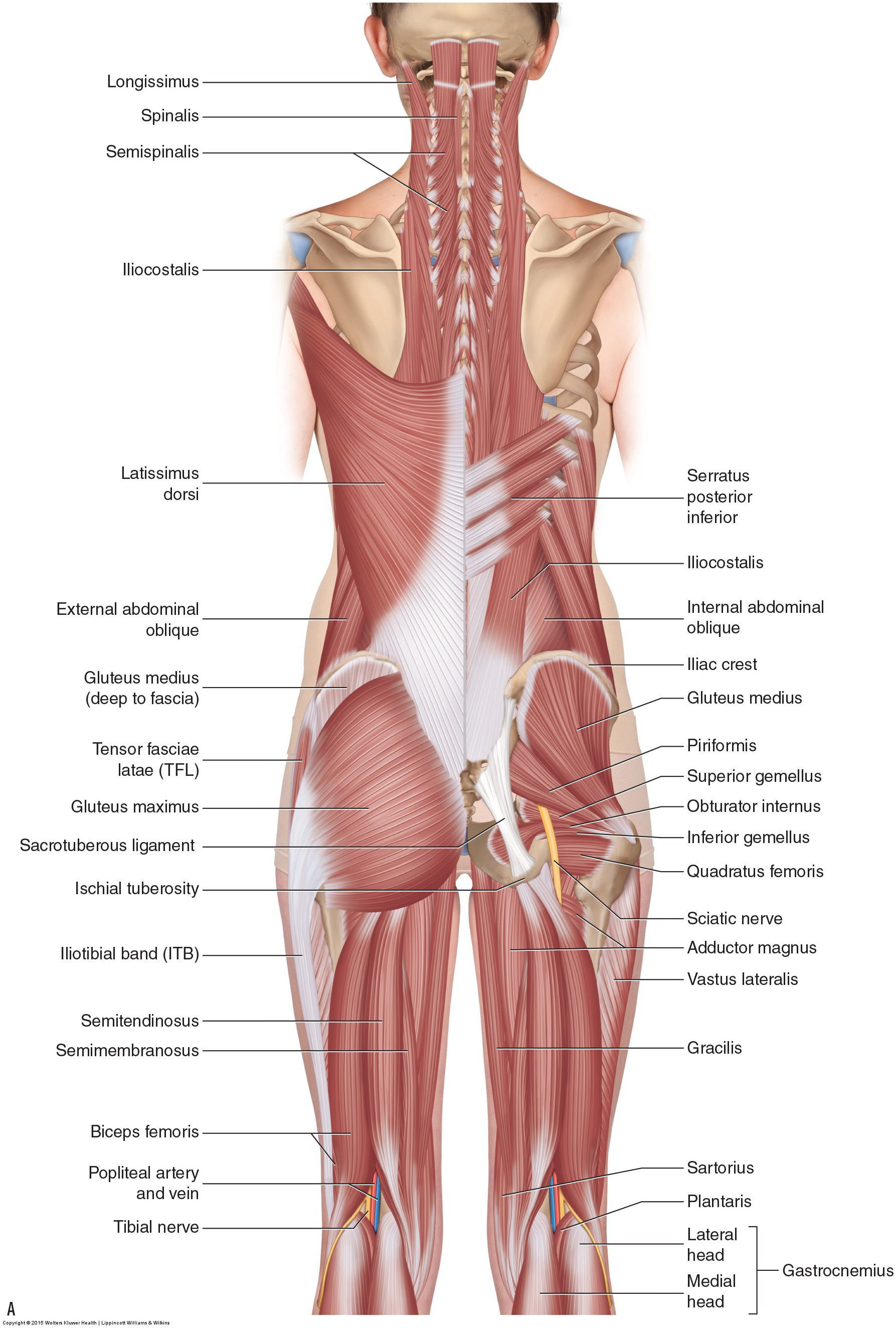
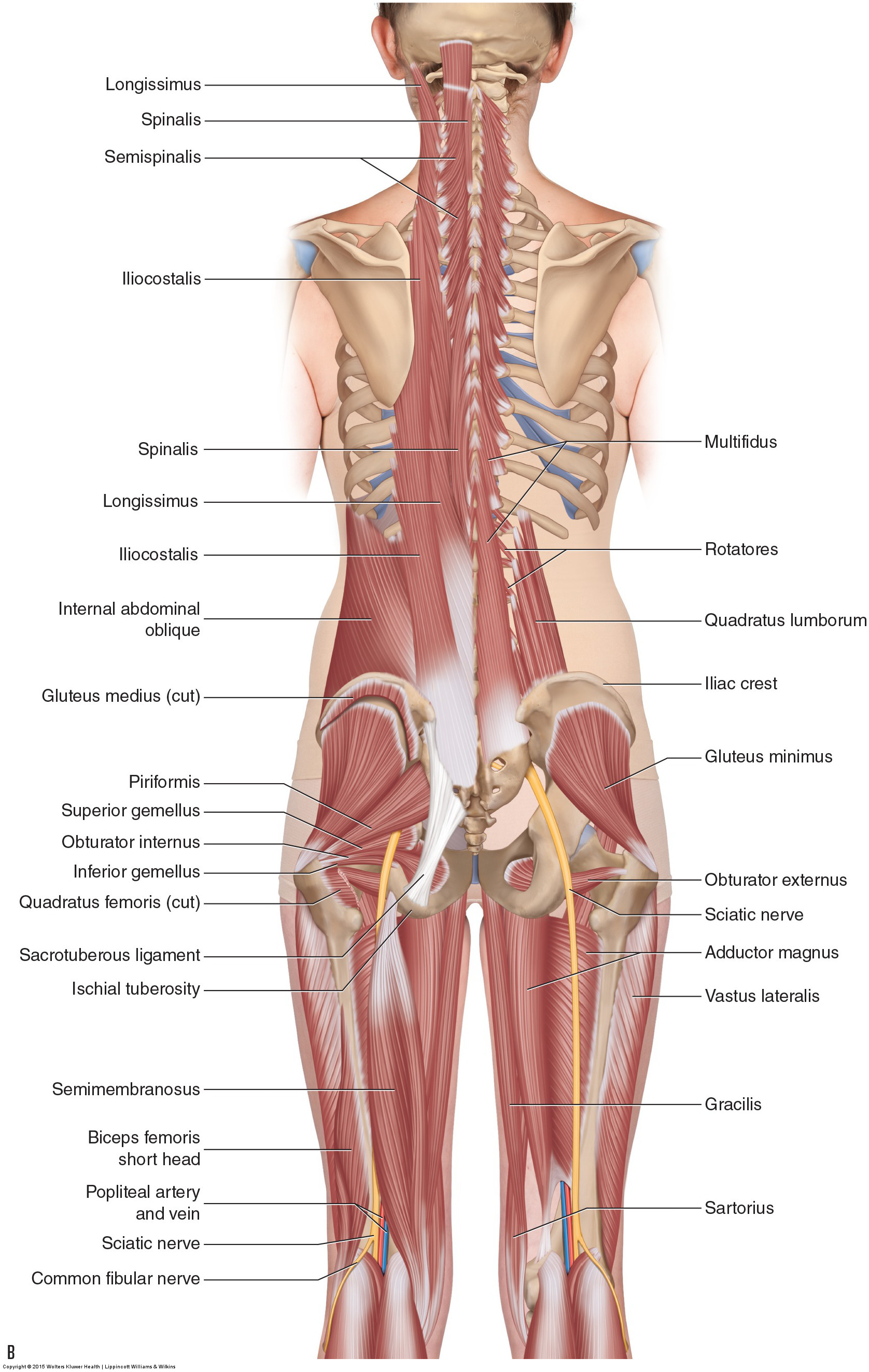
Figure 30. Posterior view of the musculature of the low back and pelvis region. (A) Superficial view on the left with an intermediate view on the right. (B) Deeper set of views. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).

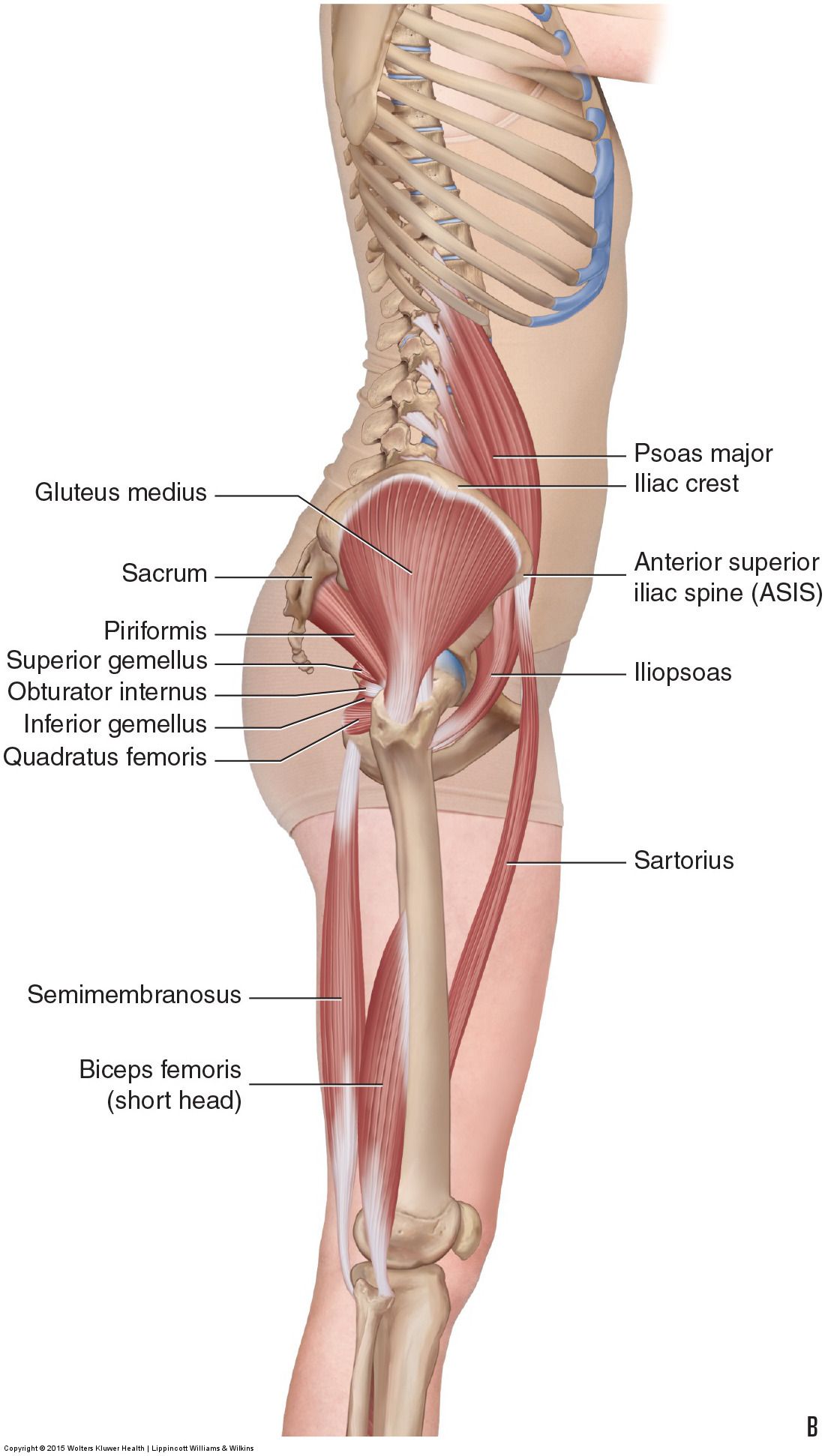
Figure 31. Right lateral views of the musculature of the low back and pelvis region. (A) Superficial view. Deeper view. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
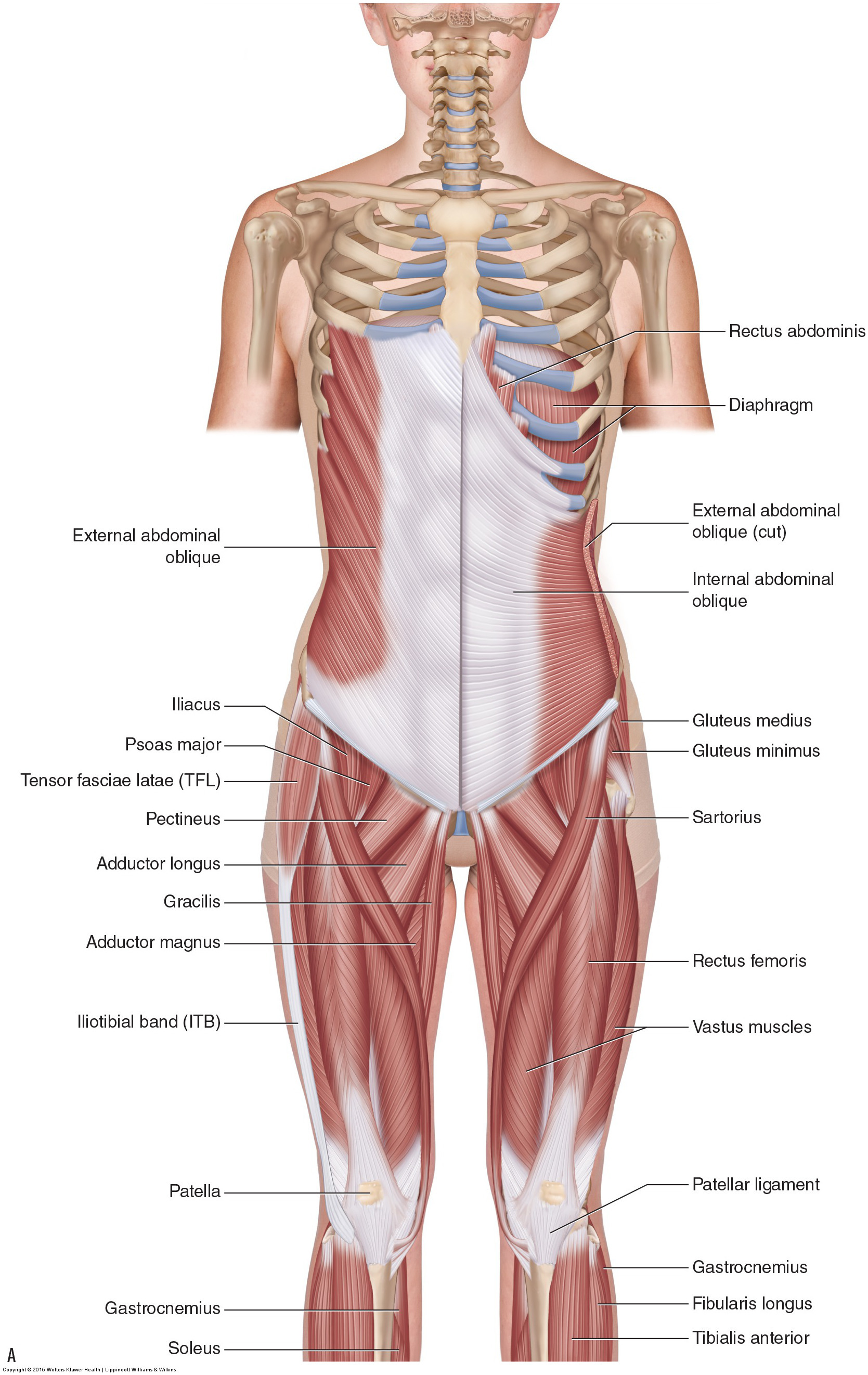
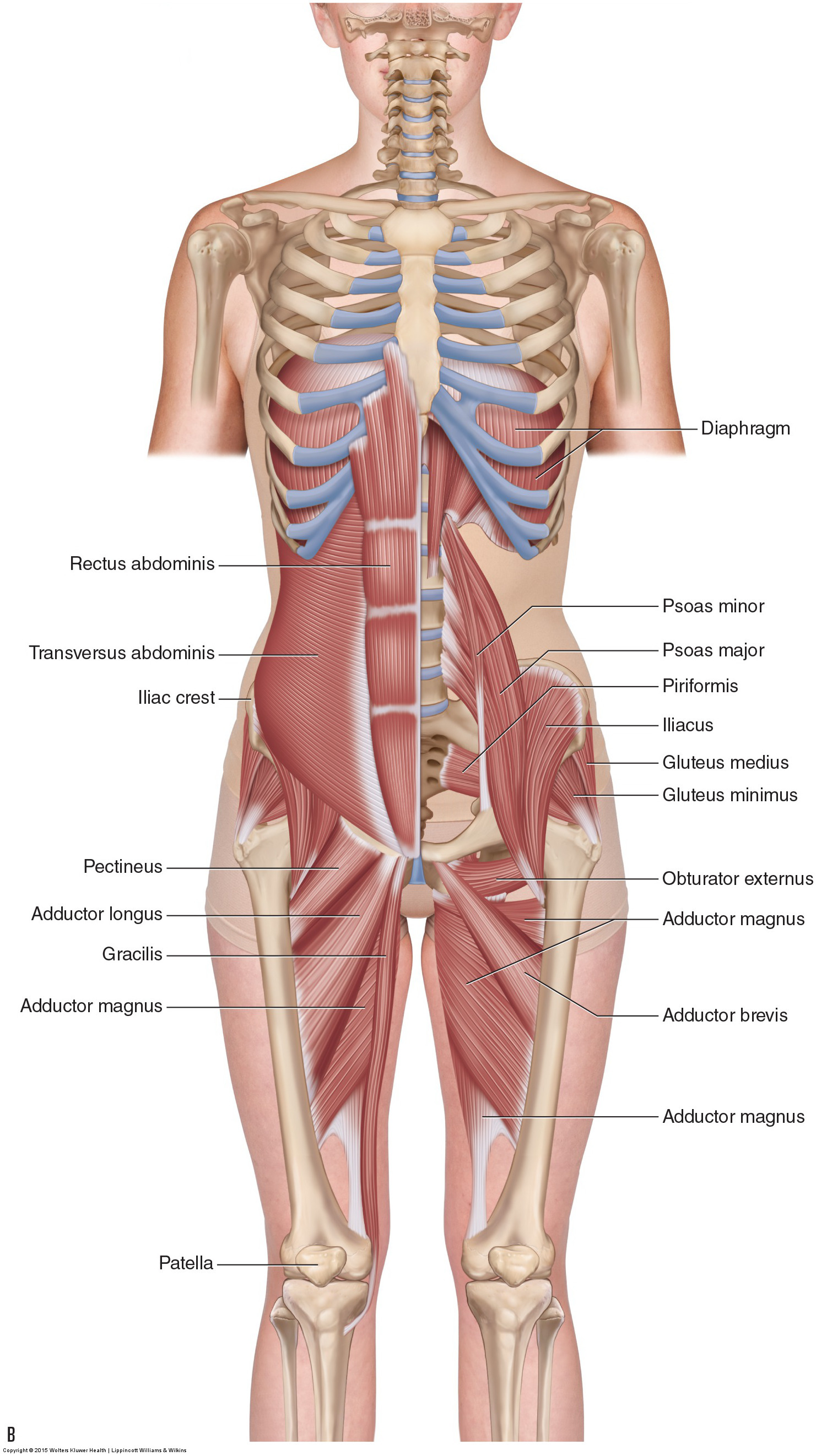
Figure 32. Anterior views of the musculature of the low back and pelvis region. (A) Superficial view on the right with an intermediate view on the left. (B) Deeper set of views. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Pelvic Muscles that Cross the Lumbosacral Joint and Attach onto the Trunk
Muscles of the pelvis that cross the lumbosacral joint to attach onto the trunk were described in the previous blog post article on “Muscles of the Trunk.” Their reverse action pelvic motions occur when their superior trunk attachment is fixed, and the pelvic attachment moves instead. Given that they are the same trunk muscle groups simply looked at from the perspective of their pelvic action, they can also be divided into the same four quadrants. The anterior muscles posteriorly tilt the pelvis, the posterior muscles anteriorly tilt the pelvis, the muscles on the right side elevate the right side of the pelvis (and therefore depress the left side of the pelvis), and the muscles on the left side elevate the left side of the pelvis (and therefore depress the right side of the pelvis).
As with the discussion of these muscles from the perspective of the trunk, understanding pelvic rotation motions by these muscles requires visualizing the horizontal component to the fiber direction of the muscles. Alternately, you simply realize that because these are reverse actions, if a muscle rotates the trunk in one direction, it must rotate the pelvis in the opposite (reverse) direction. See Table 3 for more information on this.
Pelvic Muscles that Cross the Hip Joint and Attach onto the Thigh/Leg
Muscles that cross the hip joint are usually thought of with respect to their open chain motion of the thigh relative to the pelvis at the hip joint. As such, you can also divide the musculature that moves the thigh at the hip joint into quadrants. The flexors are located anteriorly, extensors posteriorly, abductors laterally, and adductors medially. Rotation musculature is not as easily equated with location; however, as a general rule, lateral rotators are located posteriorly and medial rotators are located anteriorly. However, looking at these muscles’ open chain actions on the thigh is not as important as understanding their closed chain actions on the pelvis. This is crucially important because the foot is so often on the ground, causing closed chain kinematic pelvic motion. Posture and motion of the pelvis then have repercussions on spinal posture and motion. See Table 2 for more information on the standard/reverse actions of the thigh and pelvis at the hip joint for these muscles. Following are hip joint muscles of the pelvis.
Figures 33 through 42 illustrate the individual muscles and muscle groups of the pelvis at the hip joint along with their specific attachment and action information. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
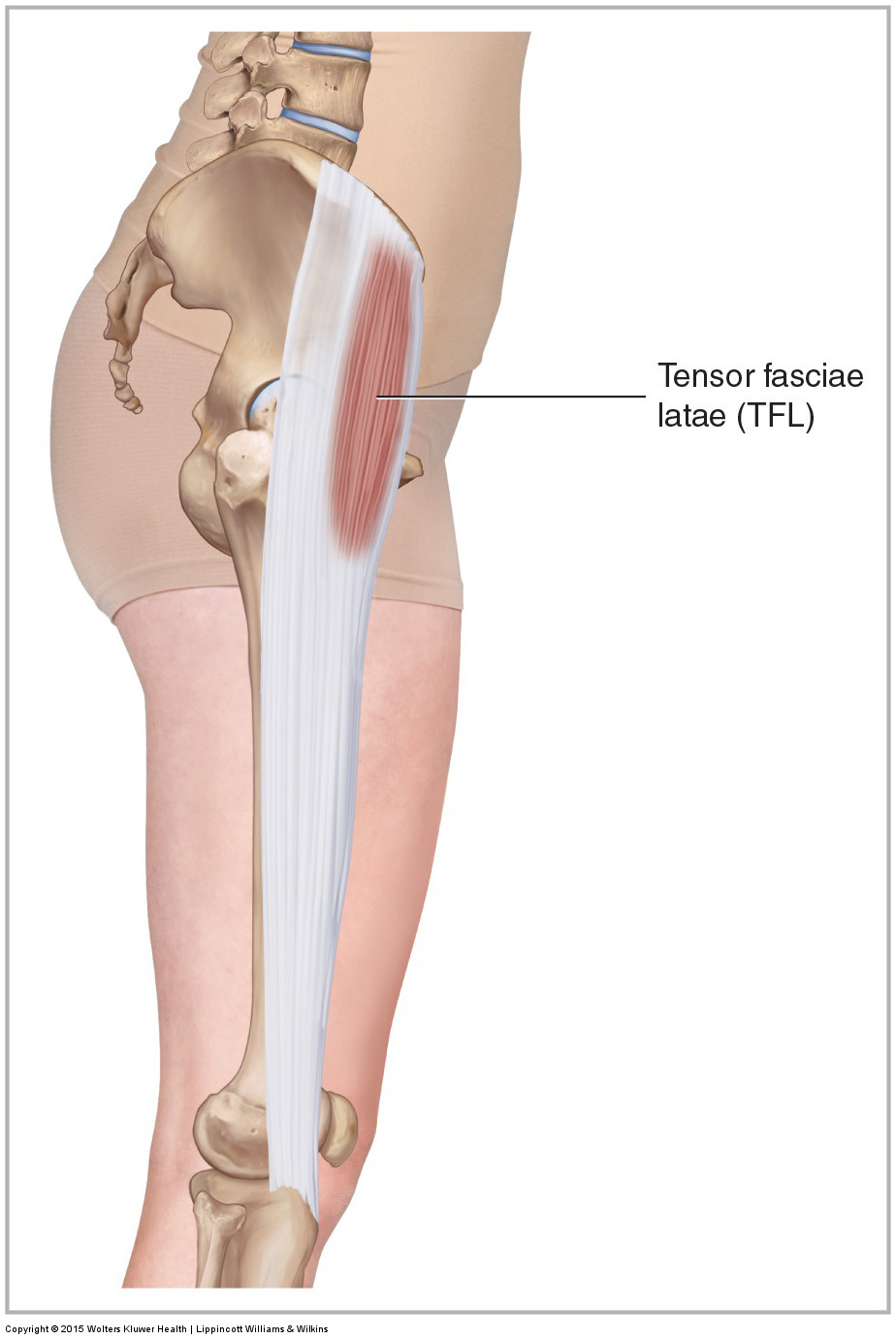
Figure 33. Lateral view of the right tensor fasciae latae (TFL). Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Tensor Fasciae Latae
- The tensor fasciae latae (TFL) attaches from the ASIS and anterior iliac crest to the iliotibial band (ITB), one-third of the way down the thigh.
- The TFL flexes, abducts, and medially rotates the thigh at the hip joint and anteriorly tilts and depresses the same-side pelvis at the hip joint.
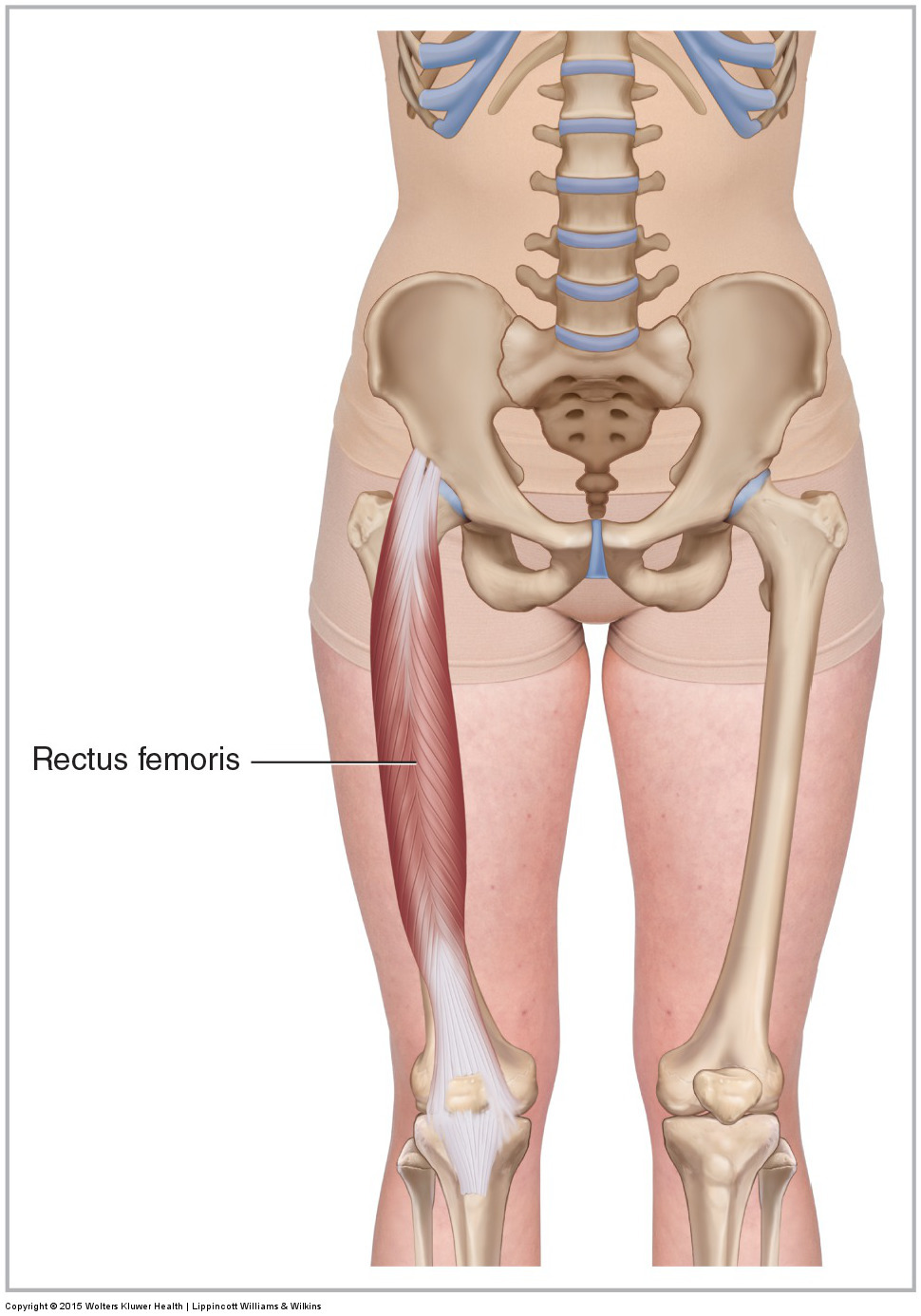
Figure 34. Anterior view of the right rectus femoris of the quadriceps femoris group. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Rectus Femoris
- The rectus femoris of the quadriceps femoris group attaches from the AIIS to the patella and then onto the tibial tuberosity via the patella ligament.
- The rectus femoris flexes the thigh at the hip joint and anteriorly tilts the pelvis at the hip joint. It also extends the leg (and/or thigh) at the knee joint.
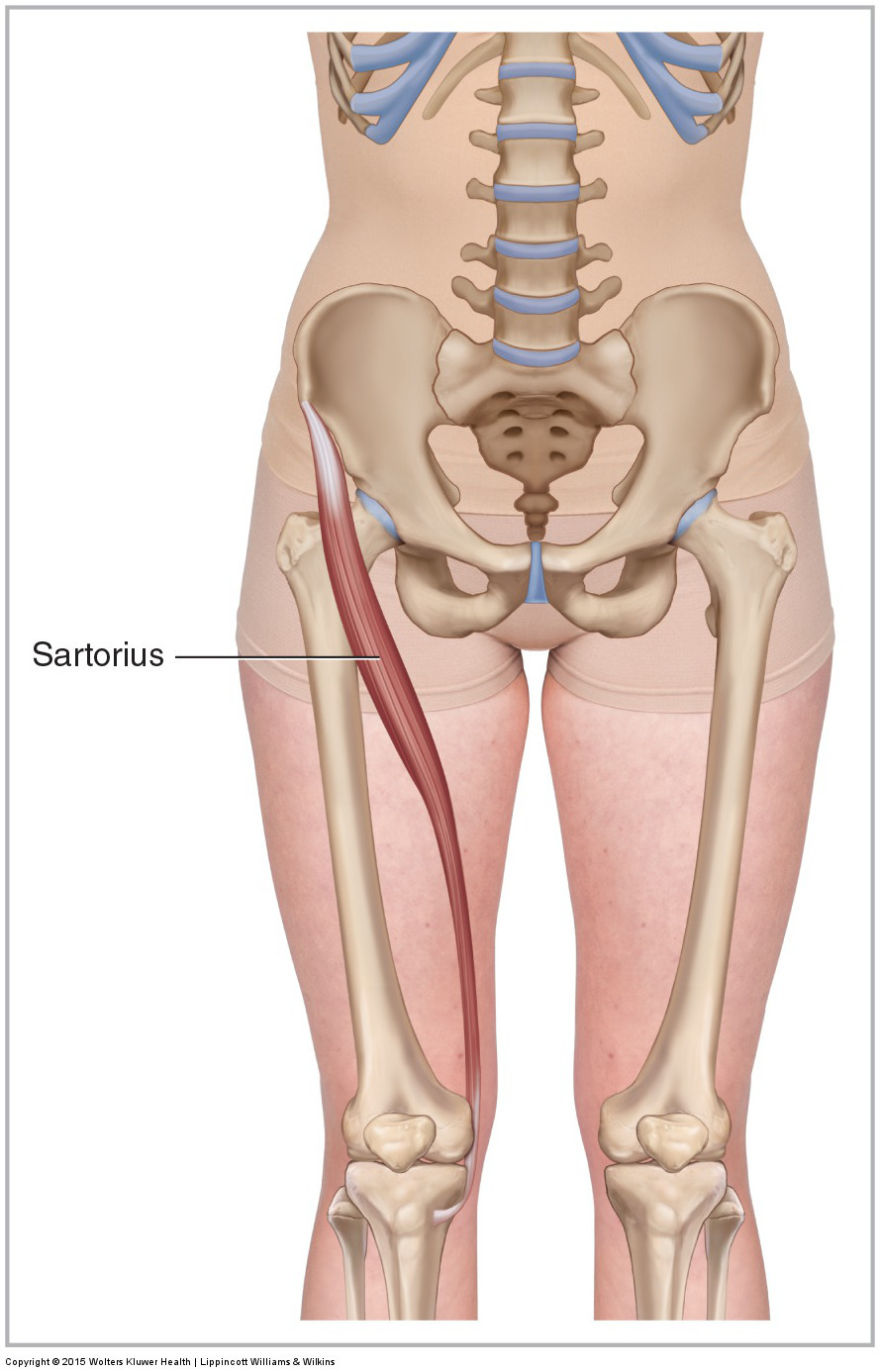
Figure 35. Anterior view of the right sartorius. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Sartorius
- The sartorius attaches from the ASIS to the pes anserine tendon at the proximal anteromedial tibia.
- The sartorius flexes, abducts, and laterally rotates the thigh at the hip joint and anteriorly tilts the pelvis and depresses the same-side pelvis at the hip joint. It also flexes the leg (and/or thigh) at the knee joint.
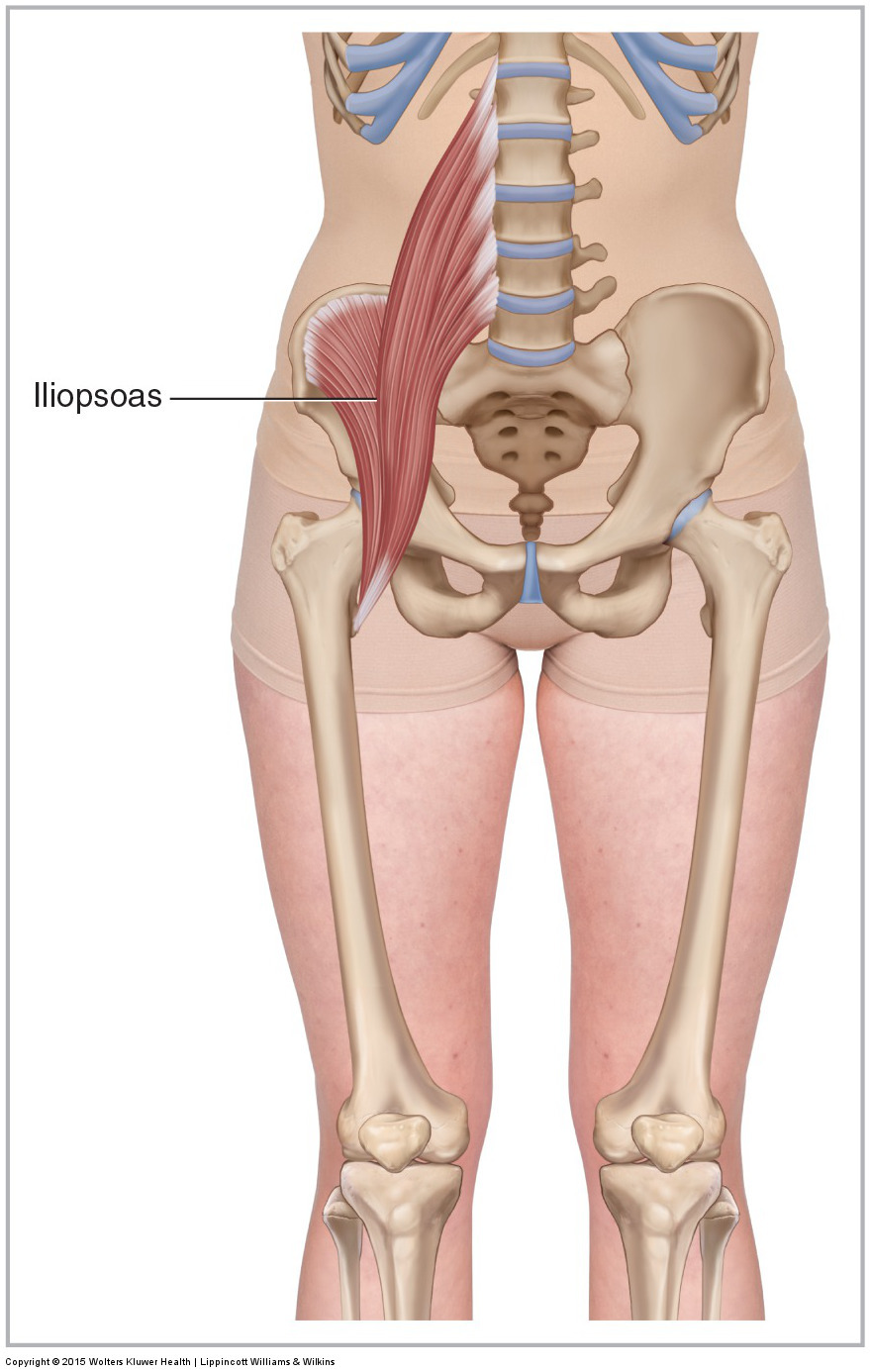
Figure 36. Anterior view of the right iliopsoas muscle. The iliopsoas is composed of the iliacus and psoas major muscles. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Iliopsoas
- The psoas major of the iliopsoas attaches from the anterolateral bodies and discs of T12-L5 and transverse processes of L1-L5 to the lesser trochanter of the femur. The iliacus of the iliopsoas attaches from the internal surface of the ilium to the lesser trochanter of the femur.
- Both the psoas major and iliacus flex and laterally rotate the thigh at the hip joint and anteriorly tilt the pelvis at the hip joint. The psoas major also flexes, laterally flexes, and contralaterally rotates the trunk at the spinal joints.
Note: For much more on psoas major function, there is a series of blog post articles on learnmuscles.com. The first article in this series can be accessed by clicking here (from there, the other 10 blog post articles in the series can be accessed).
(Note: Click here for a video on iliacus function.)
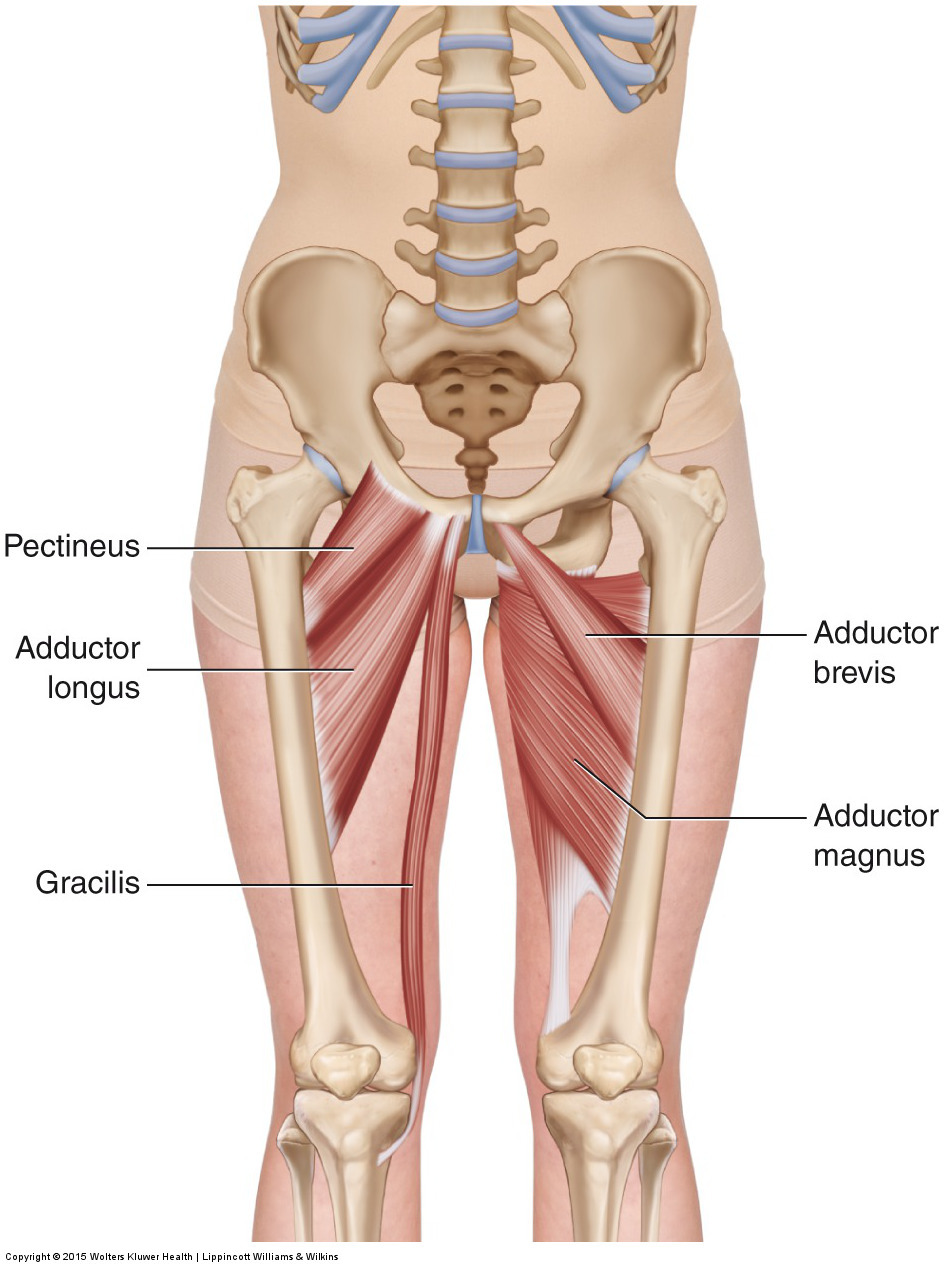
Figure 37. Anterior views of the adductor group. The adductor group is composed of the pectineus, adductor longus, adductor brevis, adductor magnus, and gracilis. The pectineus, adductor longus, and gracilis are shown on the client’s right side (left side of figure); the adductor brevis and adductor magnus are shown on the client’s left side (right side of figure). Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Adductor Group
- The adductor group attaches from the pubic bone and ischium to the linea aspera, pectineal line, adductor tubercle of the femur, and the pes anserine tendon at the proximal anteromedial tibia.
- As a group, the adductors adduct, flex, and medially rotate the thigh at the hip joint and anteriorly tilt and ipsilaterally rotate (and elevate the same-side) pelvis at the hip joint. The gracilis can also flex the leg (and/or thigh) at the knee joint. The adductor magnus extends the thigh and posteriorly tilts the pelvis at the hip joint.
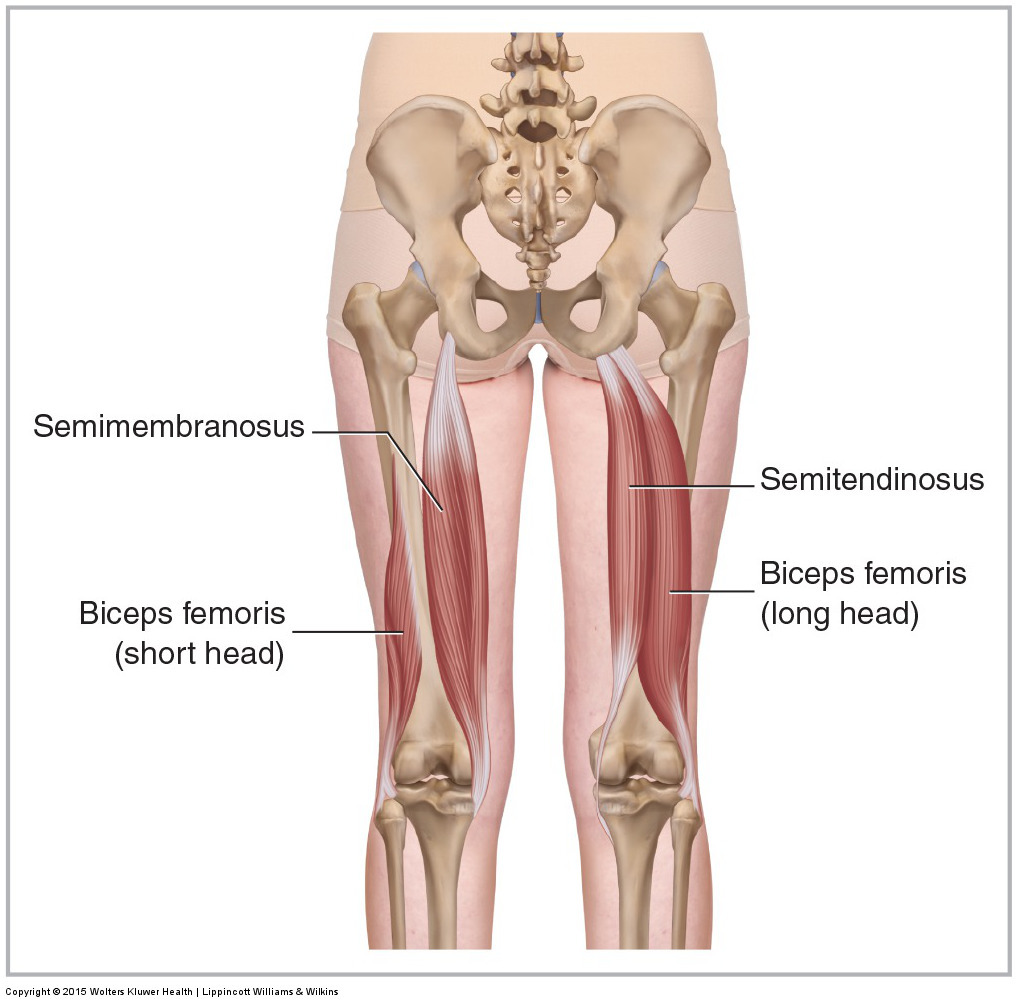
Figure 38. Posterior views of the hamstring group. The hamstring group is composed of the semitendinosus and semimembranosus medially and the biceps femoris laterally. The semitendinosus and long head of the biceps femoris are shown on the right side; the deeper semimembranosus and short head of the biceps femoris are shown on the left side. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Hamstring Group
- The biceps femoris attaches from the ischial tuberosity (long head) and linea aspera of the femur (short head) to the head of the fibula. The semitendinosus attaches from the ischial tuberosity to the pes anserine tendon at the proximal anteromedial tibia. The semimembranosus attaches from the ischial tuberosity to the posterior surface of the medial condyle of the tibia.
- As a group, the hamstrings extend the thigh and posteriorly tilt the pelvis at the hip joint. They also flex the leg (and/or thigh) at the knee joint. (Note: The short head of the biceps femoris does not cross the hip joint and therefore has no action at that joint.)
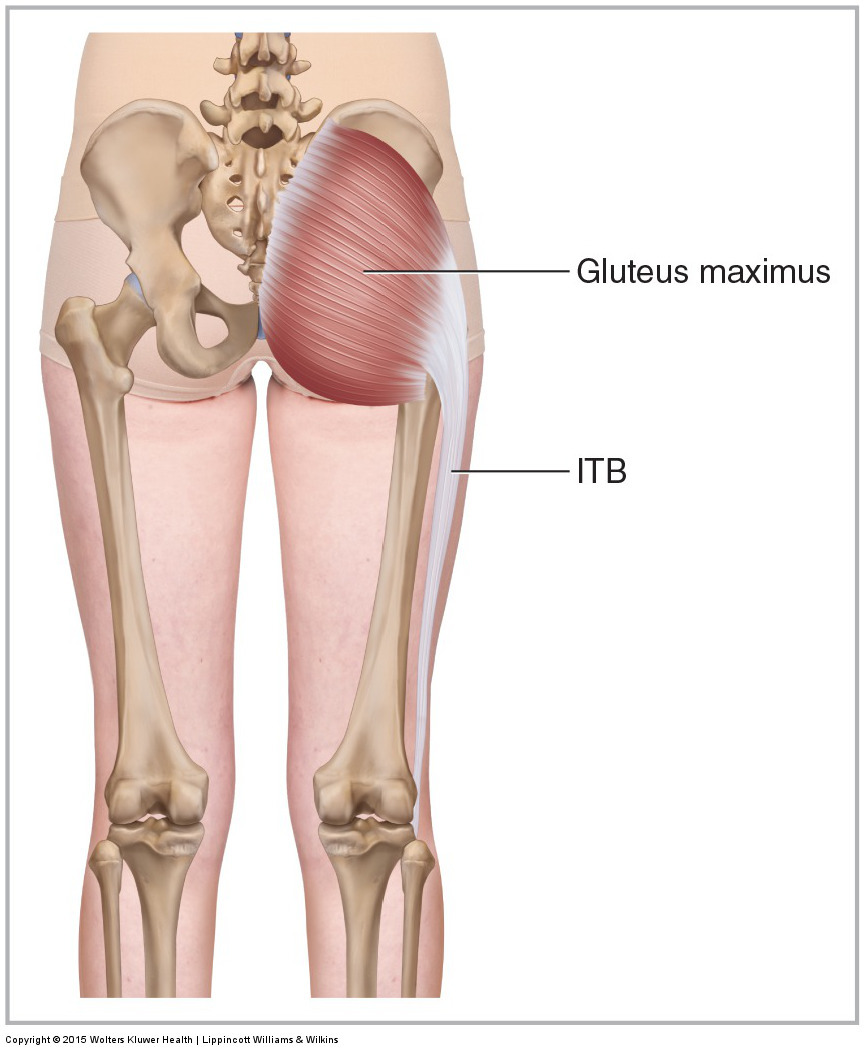
Figure 39. Posterior view of the right gluteus maximus. ITB, iliotibial band. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Gluteus Maximus
- The gluteus maximus attaches from the posterior iliac crest, posterolateral sacrum, and coccyx to the gluteal tuberosity and ITB.
- The gluteus maximus extends, laterally rotates, abducts (upper fibers), and adducts (lower fibers) the thigh at the hip joint. It also posteriorly tilts and contralaterally rotates the pelvis at the hip joint.
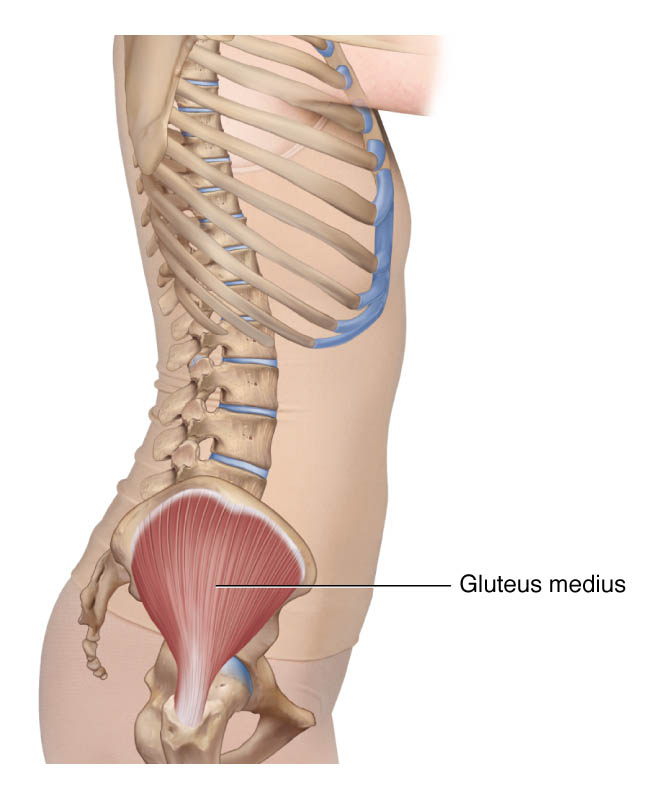
Figure 40. Lateral view of the right gluteus medius. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Gluteus Medius
- The gluteus medius attaches from the external ilium to the greater trochanter of the femur.
- The entire gluteus medius abducts the thigh at the hip joint and depresses the same-side pelvis at the hip joint. The anterior fibers also flex and medially rotate the thigh and anteriorly tilt and ipsilaterally rotate the pelvis at the hip joint; the posterior fibers also extend and laterally rotate the thigh and posteriorly tilt and contralaterally rotate the pelvis at the hip joint.
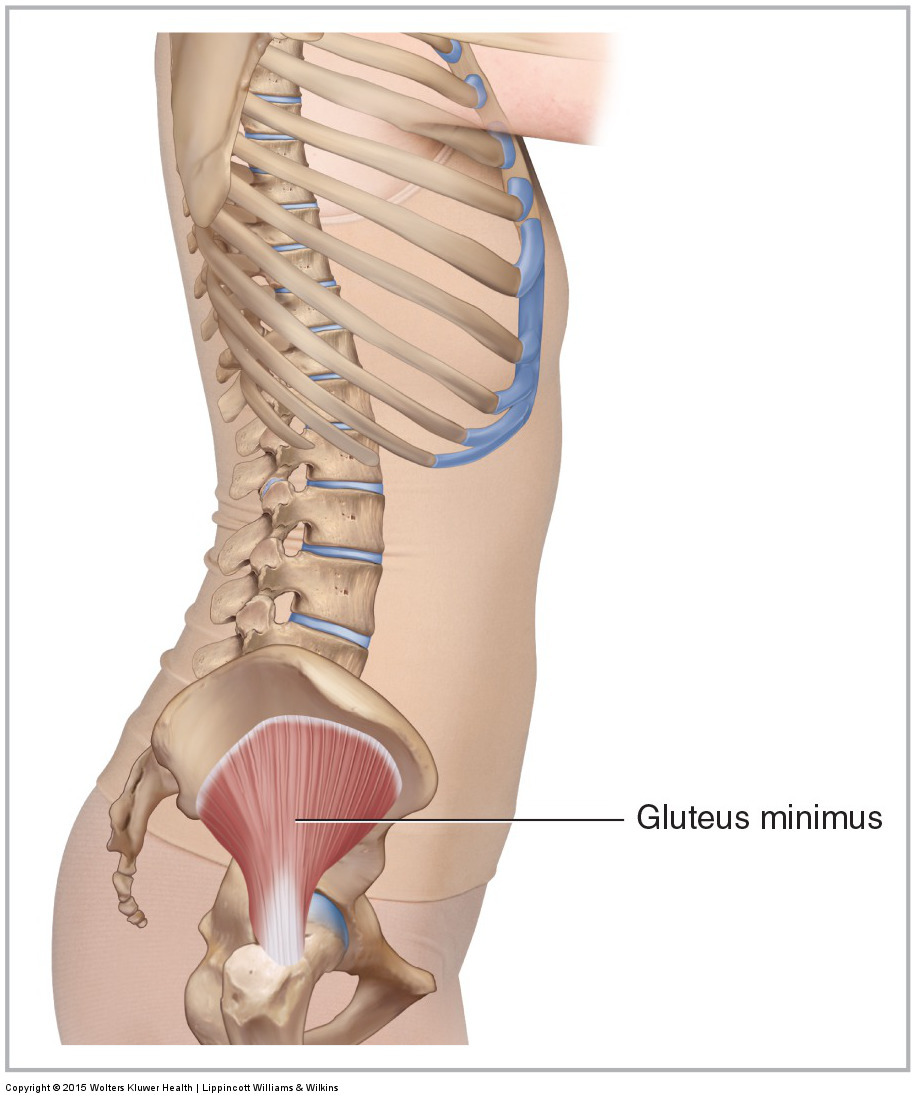
Figure 41. Lateral view of the right gluteus minimus. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Gluteus Minimus
- The gluteus minimus attaches from the external ilium to the greater trochanter of the femur (Note: The gluteus minimus is located deep to the gluteus medius).
- The entire gluteus minimus abducts the thigh at the hip joint and depresses the same-side pelvis at the hip joint. The anterior fibers also flex and medially rotate the thigh and anteriorly tilt and ipsilaterally rotate the pelvis at the hip joint; the posterior fibers also extend and laterally rotate the thigh and posteriorly tilt and contralaterally rotate the pelvis at the hip joint.
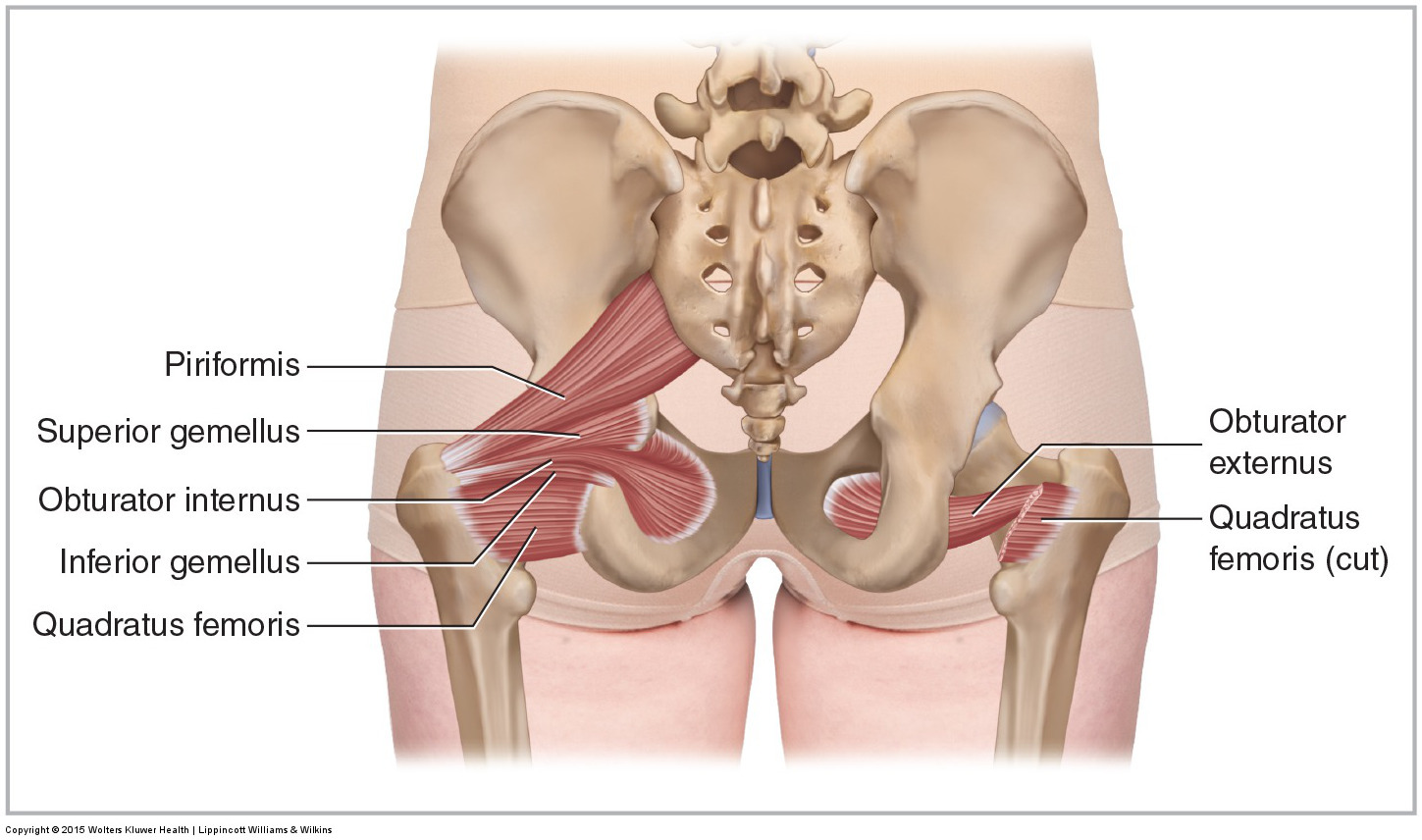
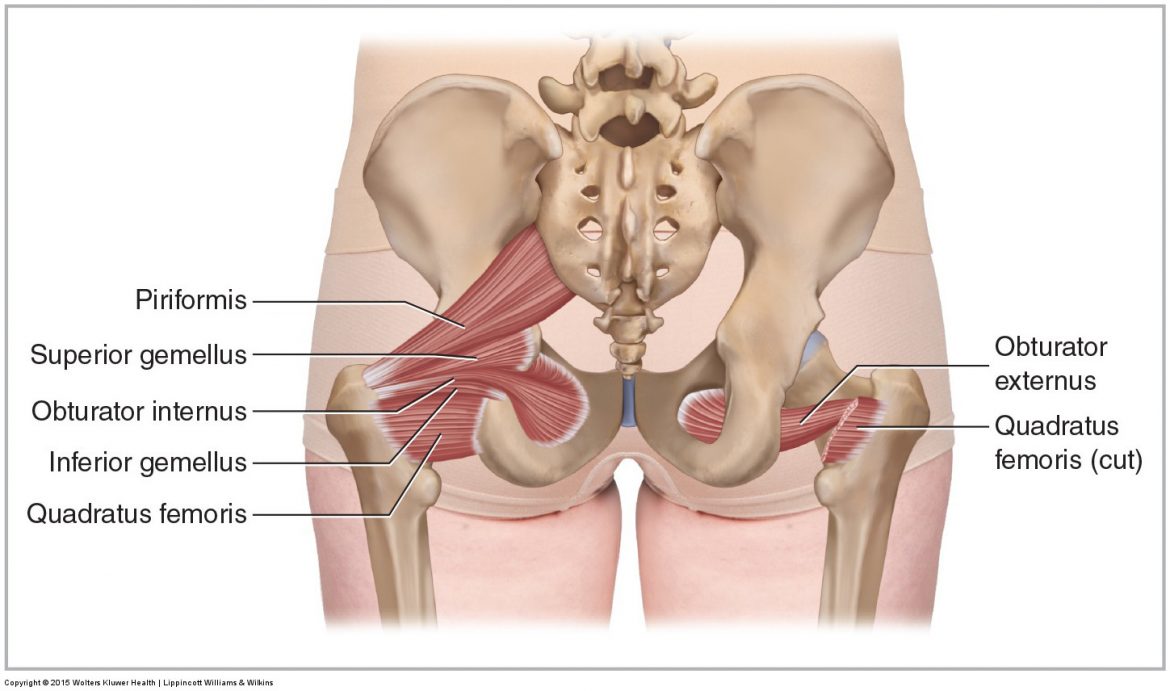
Figure 42. Posterior view of the deep lateral rotator group. All muscles of the group are drawn on the left side (the obturator externus is not seen). The quadratus femoris has been cut on the right side to visualize the obturator externus. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Deep Lateral Rotator Group
- The deep lateral rotator group attaches from the sacrum (piriformis) and the pelvic bone (the rest of the group) to the (or nearby the) greater trochanter of the femur.
- As a group, the deep lateral rotators laterally rotate the thigh at the hip joint and contralaterally rotate the pelvis at the hip joint. If the thigh is first flexed to 90 degrees, the deep lateral rotators can horizontally extend (horizontally abduct) the thigh at the hip joint. Note: If the thigh is first flexed (approximately 60 degrees or more), the piriformis changes to become a medial rotator of the thigh at the hip joint instead of a lateral rotator.
(Note: Click here for a 3D Animation on Piriformis function.)
(Note: Click here for an article on Piriformis Syndrome.)
(Note: Click here for an article on the Quadratus Femoris muscle.)
Note: Femoropelvic Rhythm
The term femoropelvic rhythm is used to describe the coordinated rhythm to how the femur and pelvis move. For example, when flexing the thigh at the hip joint to lift the foot up into the air anteriorly, the brain usually co-orders the pelvis to drop into posterior tilt because this facilitates bringing the foot even higher. Therefore, by femoropelvic rhythm, thigh flexion couples with pelvic posterior tilt. Similarly, thigh extension couples with pelvic anterior tilt. (Note: Femoropelvic rhythm is not the same as reverse actions at the hip joint. For example, the reverse action of thigh flexion at the hip joint is anterior pelvic tilt [not posterior pelvic tilt as with femoropelvic rhythm] at the hip joint).
Pelvic Floor Muscles Wholly Located Within the Pelvis
Muscles of the pelvic floor do not cross from the pelvis to another body part; therefore, they do not move the pelvis as a unit relative to the trunk or thighs. Rather, their function is primarily to stabilize the sacroiliac and symphysis pubis joints as well as to create a stable floor for the visceral contents of the abdominopelvic cavity.
Figure 43 illustrates the muscles of the pelvic floor. Pelvic floor work is often performed intrarectally or intravaginally and is therefore usually beyond the scope of practice for most manual therapists. However, some pelvic floor musculature (coccygeus and levator ani) are partially accessible from the outside, inferior to the piriformis.
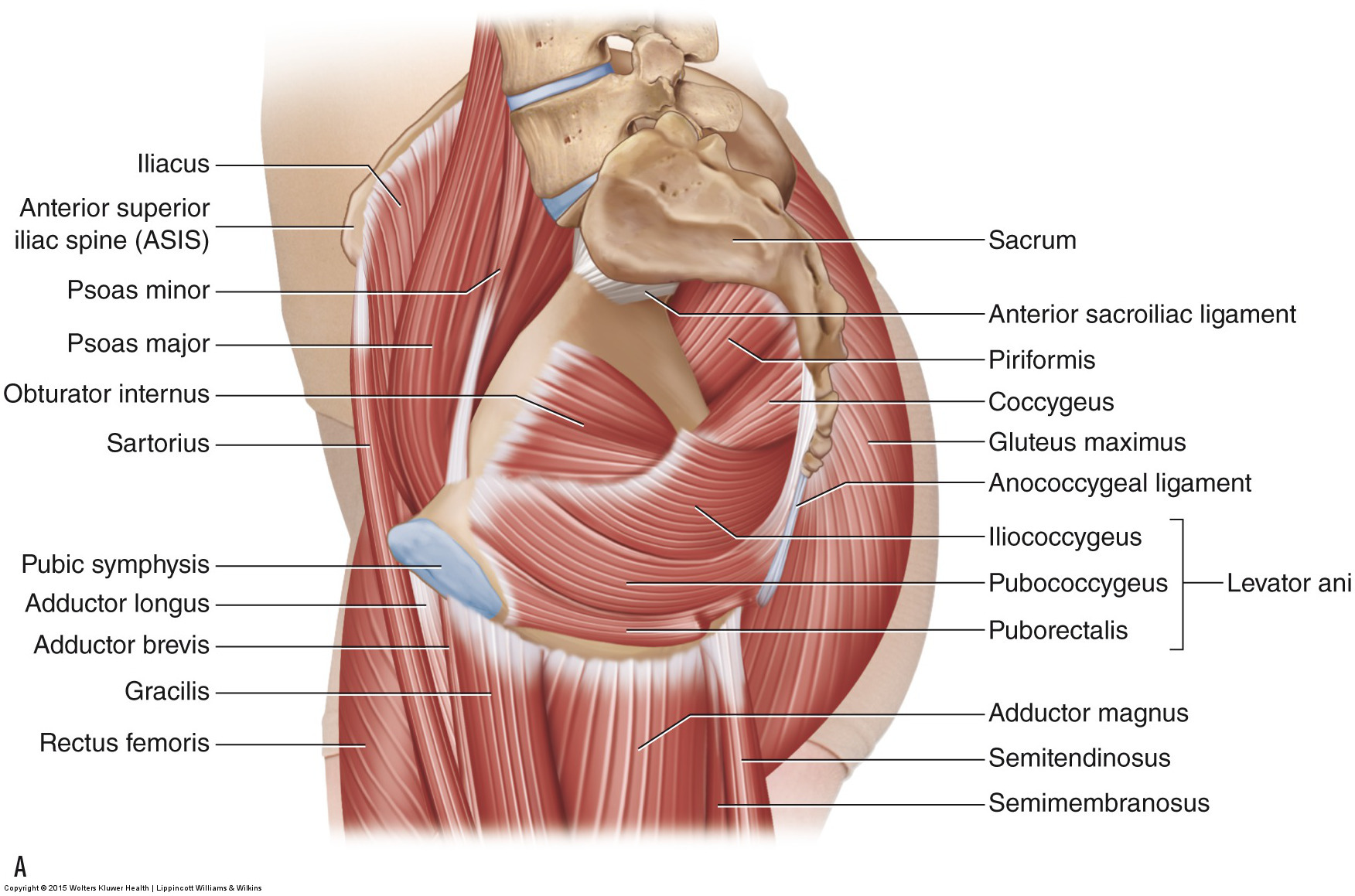
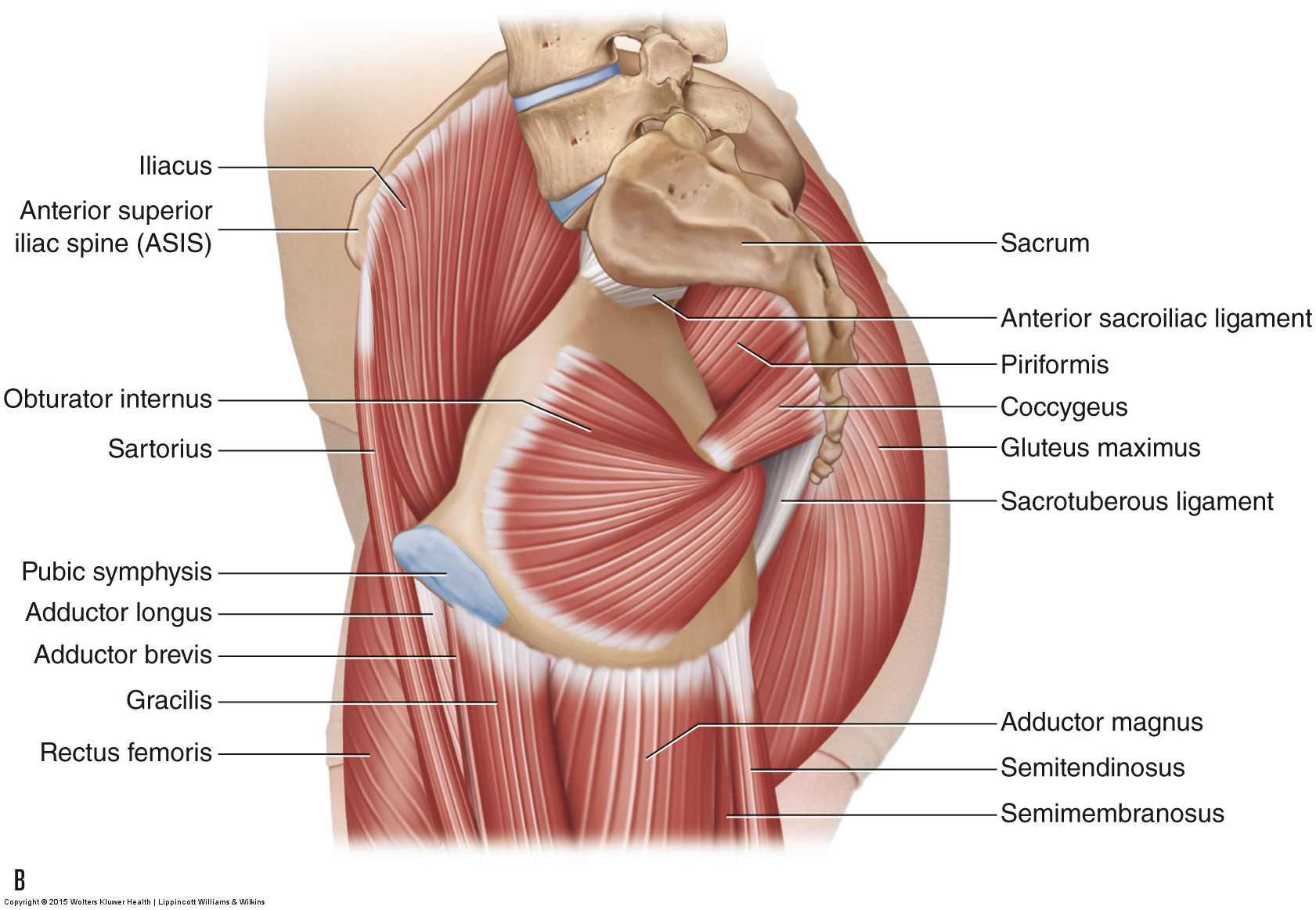
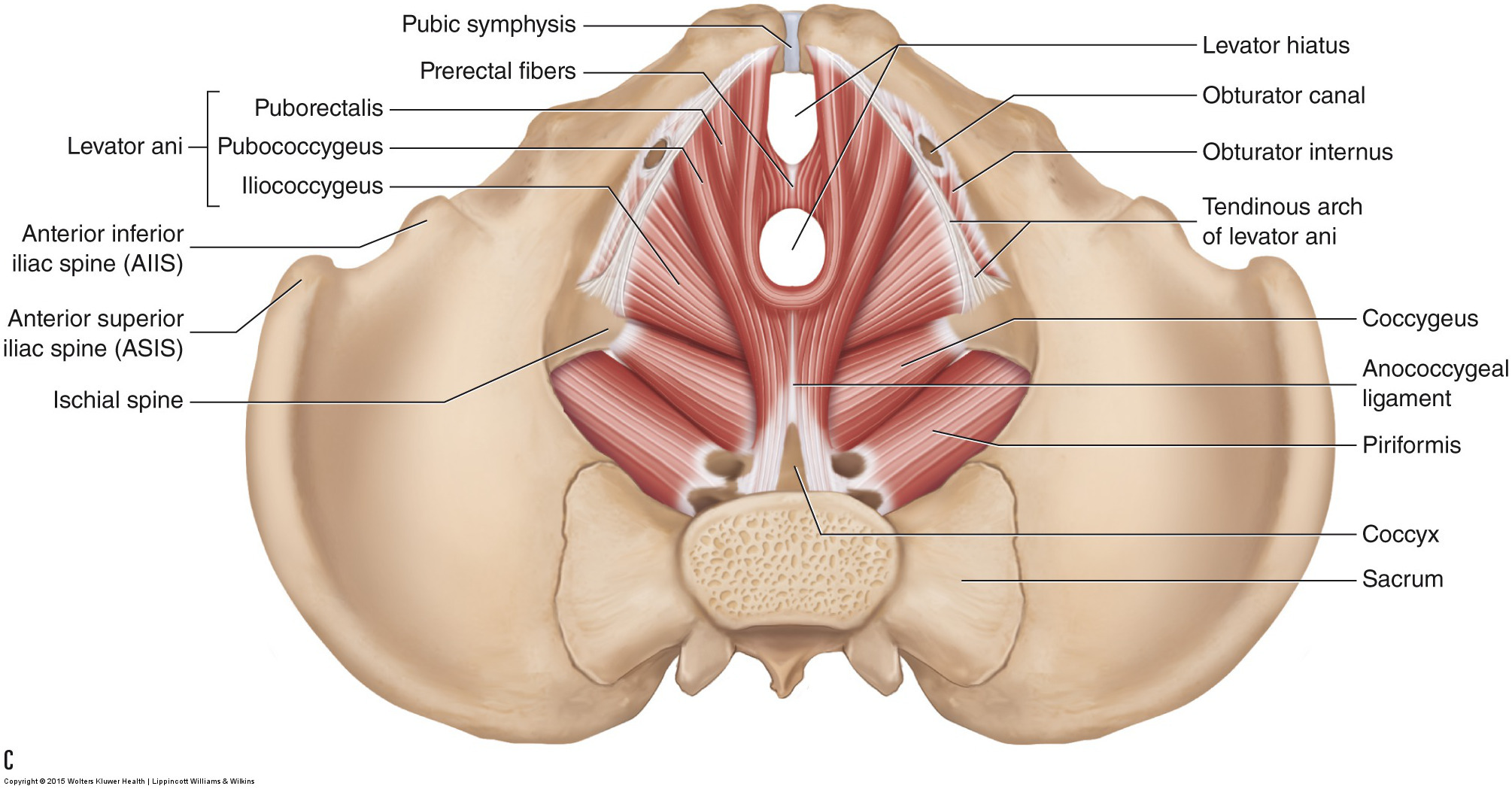
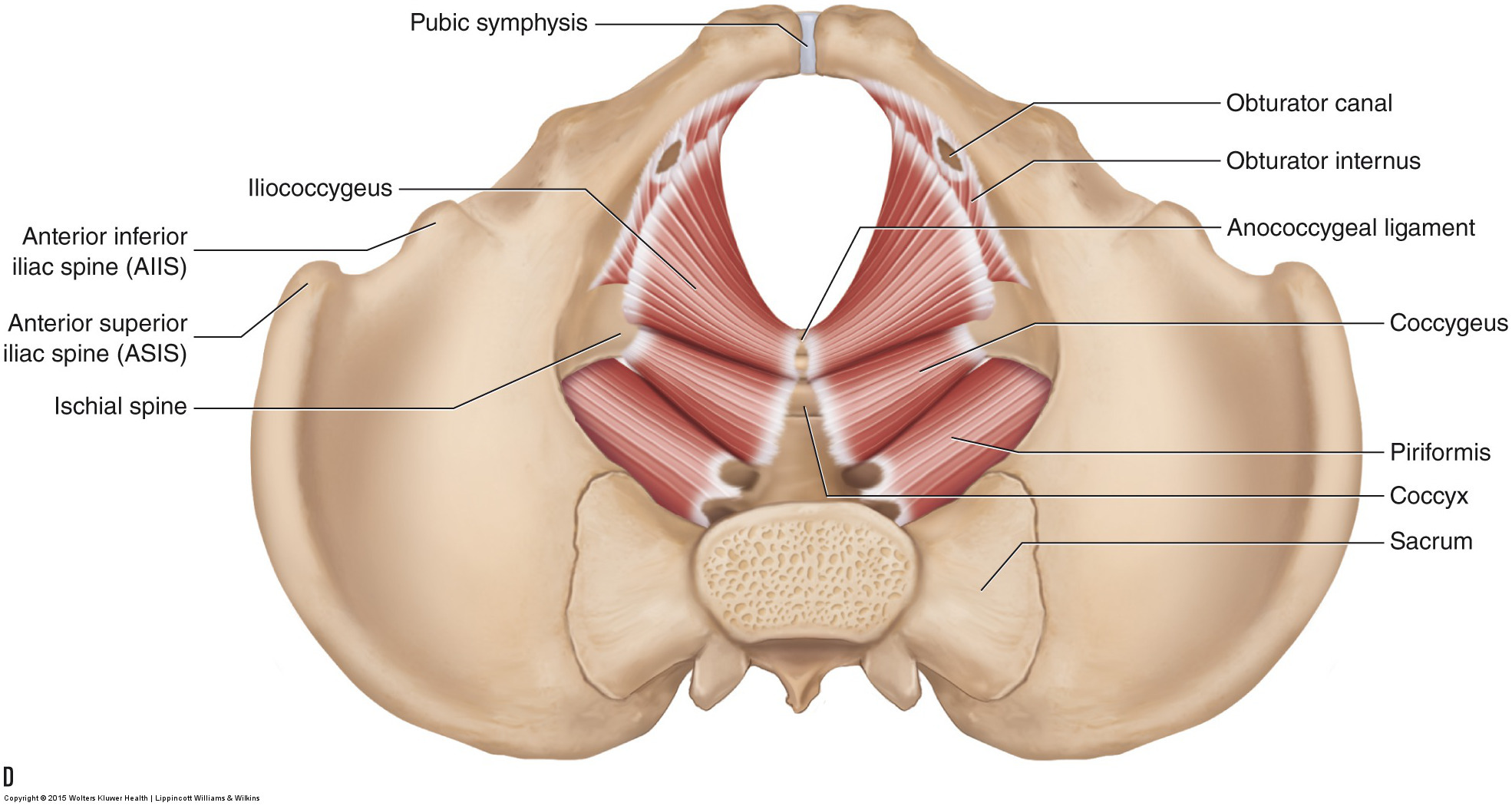
Figure 43. The muscles of the pelvic floor. (A, B) Medial views of the right side of the pelvis. (A) Superficial. (B) Deep. (C, D) Superior views of the muscles of the female pelvic floor. (C) Superficial. (D) Deep. Courtesy Joseph E. Muscolino. Manual Therapy for the Low Back and Pelvis – A Clinical Orthopedic Approach (2015).
Note: This is the sixth in a series of 8 blog post articles on the anatomy and physiology of the lumbar spine and pelvis.
The blog post articles in this series are:
- Bones of the Lumbar Spine and Pelvis
- Joints of the Lumbar Spine (disc & facet) and Pelvis
- Motions of the Joints of the Lumbar Spine
- Motions of the Joints of the Pelvis
- Muscles of the Lumbar Spine
- Muscles of the Pelvis
- Ligaments of the Lumbar Spine and Pelvis
- Precautions for Manual Therapy of the Lumbar Spine and Pelvis
